AUCTORES
Globalize your Research

Review Article | DOI: https://doi.org/10.31579/2637-8892/315
Educational and Scientific Institute of Postgraduate Education of Kharkiv National Medical University, Ukraine
*Corresponding Author: Garnik S. Kocharyan, Educational and Scientific Institute of Postgraduate Education of Kharkiv National Medical University, Ukraine.
Citation: Garnik S. Kocharyan (2024), Sexual Disorders in ICD-11. Innovations and their Discussion, Psychology and Mental Health Care, 8(10): DOI:10.31579/2637-8892/315
Copyright: © 2024, Garnik S. Kocharyan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 November 2024 | Accepted: 20 November 2024 | Published: 29 November 2024
Keywords: ICD-11; conditions related to sexual health; sexual disoders; discussion of innovations
The transition to ICD-11 was recommended by the WHO beginning from January 1, 2022. This classification went into effect on February 11, 2022. In ICD-11, all sexual disorders were excluded from the chapter "Mental, behavioural or neurodevelopmental disorders". The exception was paraphilias, which in ICD-11 are called paraphilic disorders. They were also simultaneously included into the new ICD-11 rubric “Conditions related to sexual health”. All other sexual disorders have also been included in this chapter. The following fact served as one of impulses for separation of the above chapter. LGBT activists and organizations applied to the ICD-11 project demanding to exclude this pathology from the list of mental disorders, because its presence in the above list, in their opinion, broke human rights. That application was not ignored. In ICD-11 the block F64 “Gender Identity Disorders” from ICD-10 was replaced with “Gender incongruence”. Also, gender incongruence (transgenderism) in ICD-11 was transferred from “Mental and behavioural disorders” ICD-10 to “Conditions related to sexual health”. In this way mental pathology “was turned” into the norm by means of a “depathologizing” effect of social factors. But leaders of organizations of transgenders do not like even the terminology, which reflects in the ICD-11. What do they think, the term “gender incongruence” is stigmatizing too, because it contains the word “incongruence” as one of its components. The problems, which compose the group “Conditions related to sexual health”, are present in Chapter 17 of ICD-11. These include (1) sexual dysfunctions; (2) sexual pain disorders; (3) gender incongruence; (4) changes in female genital anatomy; (5) changes in male genital anatomy; (6) paraphilic disorders; (7) adrenogenital disorders; (8) predominantly sexually transmitted infections; (9) contact with health services for contraceptive management. The article discusses aspects associated with sexual dysfunctions: the required duration of their existence for making a proper diagnosis; the obligation of presence of the diagnostic criterion, according to which a sexual problem must cause clinically significant distress; the exclusion of sexual aversion from this category; the transfer of excessive sexual drive to the Chapter “Compulsive sexual behaviour disorder”; the discussion of the problem of a normal duration of a sexual intercourse, and others. The article contains the author’s table of comparisons of sexual dysfunctions as well as sexual pain disorders in ICD-10 and ICD-11. The author informs that Chapter F66 “Psychological and behavioural disorders associated with sexual development and orientation”, which also contained egodystonic sexual orientation, was completely excluded from ICD-11. The discussion also involves partial depathologizing of paraphilias, which is based on the absence of a diagnostic criterion of the presence of distress caused by them, which is reflected in ICD-11. According to this approach, if such distress is absent and a person fully accepts the direction of his sexual drive, then we are talking about a mentally healthy person who has paraphilia, and if paraphilia is not accepted and causes distress, then this is a paraphilic disorder, which refers to mental pathology. The above is fully applied to paedophilia too. What calls attention to itself is absence of masochism among the paraphilic disorders listed above. The author believes that, from a medical point of view, the partial depathologization of paraphilias, which is reflected in ICD-11, is scientifically unfounded, a consequence of the action of exclusively social factors. Therefore, when diagnosing these disorders, it is advisable to use the traditional approach to their diagnosis.
The transition to ICD-11 was recommended by the WHO beginning from January 1, 2022. This classification went into effect on February 11, 2022. Its implementation in Ukraine is planned no earlier than 2006.
In ICD-11, all sexual disorders were excluded from the chapter "Mental, behavioural or neurodevelopmental disorders". The exception was paraphilias, which in ICD-11 are called paraphilic disorders. They were also simultaneously included into the new ICD-11 rubric “Conditions related to sexual health”. All other sexual disorders have also been included in this chapter. The following fact served as one of impulses for separation of the above chapter. LGBT activists and organizations applied to the ICD-11 project demanding to exclude this pathology from the list of mental disorders, because its presence in the above list, in their opinion, broke human rights. That application was not ignored. In ICD-11 the block F64 “Gender identity disorders” from ICD-10 was replaced with “Gender incongruence”. Also, gender incongruence (transgenderism) in ICD-11 was transferred from “Mental and behavioural disorders” ICD-10 to “Conditions related to sexual health”. In this way mental pathology “was turned” into the norm by means of a “depathologizing” effect of social factors. But leaders of organizations of transgenders do not like even the terminology, which reflects in the ICD-11. What do they think, the term “gender incongruence” is stigmatizing too, because it contains “incongruence” as one of its components. The problems, which compose the group “Conditions related to sexual health”, are present in Chapter 17 of ICD-11 (ICD-11 for Mortality and Morbidity Statistics. 2024-01). These include (1) sexual dysfunctions; (2) sexual pain disorders; (3) gender incongruence (4) changes in female genital anatomy; (5) changes in male genital anatomy; (6) paraphilic disorders; (7) adrenogenital disorders; (8) predominantly sexually transmitted infections; (9) contact with health services for contraceptive management.
In DSM-11, some changes were made concerning sexual disorders, which became the subject of our special consideration and discussion.
The following 2 criteria in the classification, which should attract our attention, appear in the general characteristics of sexual dysfunctions. In order to be regarded as sexual dysfunction the latter must persist at least a few months and be associated with a clinically significant distress (ICD-11 for Mortality and Morbidity Statistics, 2024-01). Obviously, a few months means at least three. A question arises why for diagnosing sexual dysfunction the latter must exist at least 3 months. What must the physician and the patient do when a sexual disorder persists less: wait until it may resolve on its own or register a lower quality of the patient’s life? Another question also arises: why a specialist in the field of sexual health, who has undergone occupational training, should wait so long in order to be able to make a proper diagnosis?
At first (1992), the above criterion was absent in ICD-10 (The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines, 1992), but it appeared later (1993) in Diagnostic criteria for research of ICD-10 (The ICD-10 Classification of Mental and Behavioural Disorders. Diagnostic criteria for research, 1993), though it was indicated that in order to make a diagnosis of sexual dysfunction the latter should persist at least 6 months. That regulation almost completely agreed with the one present in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (USA) published in 2013 (Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition, 2013), which contains a classification of sexual disorders, though the expression of the diagnostic criterion in the above classification is milder. Thus, it was indicated that the minimum duration of decreased sexual desire should be about 6 months. From our point of view, a lower duration of the temporal criterion in ICD-11 should be regarded as a positive fact.
Another aspect of the problem consists in a possibility to make a diagnosis of a certain sexual dysfunction only in the case when this dysfunction is associated with clinically significant distress. Before ICD-11 was approved the literature informed that ICD-11 suggested a new approach to assessment of sexual desire and activity, which paid a tribute to humanization, but hardly met the medical approach in assessment of their [removed]Kocharyan, 2021, 2024). For example, it was reported that the classification, which was being prepared, aimed at the viewpoint that there were no norms of sexual activity. It was suggested to regard as “satisfactory” such sexual activity, which satisfies this particular person. If the individual is satisfied with his/her sexual activity, the possibility to make a diagnosis of sexual dysfunction is immediately excluded, even if the above sexual activity differs from the one in other people, in other cultures or subcultures (Reed et al., 2016).
The described approach blurs the concept of norm and pathology, since any degree of expression of sexual desire and any frequency of sexual activity are considered normal. If a person with a strongly reduced or even absent sexual desire is satisfied with it and he/she does not feel any distress in this connection, then in accordance with the above regulation the person cannot be regarded as a patient. As a consequence, it is necessary to mention even the existence of the term “healthy asexuality”, which should be considered paradoxical.
However, it is quite fair to indicate that nonrealistic expectations from the side of one’s partner, inadequacy to sexual desire of the partners cannot be regarded as grounds for making a diagnosis of sexual dysfunction (Reed et al., 2016).
Hypoactive dysfunction of sexual desire is rather widely represented in the approved ICD-11 (HA00), and though one of its diagnostic criteria consists in the presence of personality distress, associated with it, we do not observe such a stiff approach to its diagnosing versus the regulation, which was present on the stage of preparation of this classification.
Code F52.1 of ICD-10 (“Sexual aversion and lack of sexual enjoyment”) does not have the appropriate code in ICD-11. It should be noted that the diagnosis “sexual aversion” was not included in 2013 into DSM-5 (the modern classification, accepted in the USA) because of its rare use and absence of confirmatory studies (Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition, 2013). This disorder was not recommended for inclusion as an independent code into ICD-11 either, where, as it was explained, the above disorder would belong to the category “Sexual pain-penetration disorder” or be positioned as a separate kind of phobic disorder (Reed et al., 2016). But when this classification was published, the above pathology did not find its place in the section “Sexual pain disorders”. Also absent are special references to this pathology in the section “Anxiety and fear-related disorders” and in its separate chapters (block L1-6B0). (It should be indicated that the term “fear” is intentionally used in the new version of ICD instead of the term “phobia”, which was common for previous classifications). In our opinion, deprival of its separate diagnostic code for this pathology does not cancel its existence (Kocharyan, 2021). We have diagnosed sexual aversion on numerous occasions in our clinical practice.
Code F52.4 of ICD-10 (“Premature ejaculation”) is particularly indicative of the man’s inability to delay ejaculation for the period, sufficient for deriving enjoyment from sexual intercourse by both partners. It is also emphasized that organic causes of premature ejaculation (PE) are unlikely. These characteristics require discussion. In the first case, maybe, it should concern healthy women without anorgasmia and difficulties in achieving an orgasm. In case of anorgasmia in women any duration of sexual intercourse will not be sufficient for reaching an orgasm, and difficulties in having it will require an extremely long duration of sexual intercourse and make inadequate demands to men.
In this connection, however, we should turn to Diagnostic criteria for research of ICD-10. Here specific criteria for diagnosis are given from the glossary “Clinical Descriptions and Diagnostic Guidelines” (CDDG), which is prepared for clinicians, teachers of psychiatry and other healthcare professionals in the field of psychiatry. In the description of diagnostic criterion B “an inability to delay ejaculation sufficiently to enjoy lovemaking” item 1 informs about “an occurrence of ejaculation before or very soon after the beginning of intercourse (if a “time limit” is required: before or within 15 seconds of the beginning of intercourse)” (The ICD-10 Classification of Mental and Behavioural Disorders. Diagnostic criteria for research, 1993.). This item contrasts sharply with the title definition of criterion B (the inability to delay ejaculation long enough to achieve satisfaction from sexual intercourse), because very few sexually healthy women will be able to achieve an orgasm during the time period directly over the interval of 15 sec. By the way, DSM-5 (Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition, 2013) identifies three degrees of severity of PE: mild (ejaculation occurs approximately within 30 seconds – 1 minute after vaginal penetration); moderate (ejaculation occurs 15-30 seconds after the penetration); severe (ejaculation occurs prior to sexual activity, upon its beginning or during about 15 seconds after the penetration). In this connection, the following data can arouse interest. In August of 2007 and September of 2009 there were meetings of the Committee, formed by the International Society for Sexual Medicine (ISSM), for providing the definition of premature ejaculation. The Committee has suggested defining lifelong PE as a male sexual dysfunction characterized by ejaculation, which always or almost always occurs prior to or within about one minute of vaginal penetration. It has been indicated that this definition concerns only men with PE, which exists from the beginning of their sexual life, and is used only for heterosexual intravaginal coitus. This group of experts has also concluded that there are not enough published objective data, which would suggest definition of evidence-based acquired PE (McMahon et al., 2008; Althof et al., 2010). In this connection it is reasonable to present the definition of PE in DSM-5, where premature ejaculation is interpreted as persistent or recurrent ejaculation, which occurs in case of partner sexual activity during approximately 1 minute following vaginal penetration and before the person wishes it (Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition, 2013). Also interesting are results of the study performed by the Soviet and Russian sexual health specialist Vasilchenko G.S. (Vasilchenko, 1973), in sexually healthy men using a stopwatch. The shortest sexual intercourse amounted to 1 minute 14 seconds (with 68 frictions), the longest one lasted 3 minutes 34 seconds (with 270 frictions), its average duration being equal to 2 minutes 2 seconds (with 62 frictions).
In ICD-11, PE is renamed as early ejaculation and also there are no any concrete temporal criteria, which characterize it. In DSM-5, PE is called both premature and early.
As we have noted earlier, ICD-10 emphasizes that organic causes of PE are unlikely. This statement does not satisfy clinical practice and data of scientific studies. Suffice it to recall the paracentral lobule syndrome, chronic prostatitis and other diseases, which could cause appearance of PE, as well as genetic predispositions for its appearance (Kocharyan, 2012, 2012, 2018). In particular, it should be noted that in DSM-5 (Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition, 2013) in the section, which deals with PE, prostatitis is called three times as a possible cause of premature ejaculation.
It is important to indicate that later in Diagnostic criteria for research of
ICD-10 any references to unlikeliness of organic causes of PE were absent (The ICD-10 Classification of Mental and Behavioural Disorders, 1993).
These are absent in ICD-11 too. As it was reported before, the latter separates different aetiological aspects of sexual dysfunctions and sexual pain disorders (HA40), including different somatic determination. Besides, the use of HA40 code made it necessary to include into ICD-11 as separate codes delayed ejaculation, which can be caused by somatogenic factors, rather than only by psychogenic ones, as well as retrograde ejaculation, which is caused only by effect of somatic factors. Delayed ejaculation as well as its absence is indirectly dealt with in
ICD-10 in rubric “Orgasmic dysfunction” (F52.3): “Orgasm either does not occur or is markedly delayed” (The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines, 1992).
ICD-11 does not contain rubric “Excessive sexual drive”, which was in ICD-10 (F52.7). In this connection we should point at Diagnostic criteria for research of ICD-10, which indicated that no attempt to develop research criteria for the above rubric was made, and it was recommended for the researchers, who studied that disorder, to suggest their own criteria for it (The ICD-10 Classification of Mental and Behavioural Disorders. Diagnostic criteria for research, 1993).
Instead of excessive sexual drive ICD-11 introduced code 6C72 “Compulsive sexual behaviour disorder” (CSBD). The latter is characterized by a persistent pattern of failure to control intense, repetitive sexual impulses or urges resulting in repetitive sexual behaviour. The symptoms may include repetitive sexual actions, which occupy a central place in the person’s life to the extent that he/she neglects his/her health and personal hygiene or other interests, occupations and duties, as well as numerous unsuccessful attempts to significantly reduce his/her repetitive sexual behavior, because the latter is accompanied with unfavourable consequences or derivation of little or no pleasure from it. The inability to control intense sexual impulses or urges and repetitive sexual behavior, caused by them, manifests during a long period of time (e.g., 6 months or more) and produces significant distress or considerable disturbances in one’s personal, family, social, educational, professional or other important areas of functioning.
ICD-11 does not have such codes as “hypersexuality” and “sexual addiction”. It should be noted that at present hypersexuality is considered as:
(1) a type of obsessive-compulsive disorder (OCD) or “OCD spectrum disorder”; (2) sexual addiction (Carnes, 1983; Orford, 1985; Weiss, 1998); (3) disorder of impulsivity that, according to Barth and Kinder (1987), in fact is an impulse control disorder (Irons et al, 1996).
At the present moment, maybe, it is possible to point out one more conceptualization of behavioural hypersexuality. For example, some authors separate persistent sexual arousal syndrome (PSAS), which was later called persistent genital arousal disorder (PGAD) (Goldmeier, Leiblum, 2006; Leiblum, Nathan, 2001) as well as restless genital syndrome (ReGS) (Waldinger et al., 2009, 2010). These disorders, which, as a result, manifest themselves through significant sexual activity, were for the first time in the post-Soviet states presented in detail in my articles and my book (Kocharyan, 2015, 2015, 2015, 2020).
It should be noted that in ICD-11 sexual pain disorders were separated from sexual dysfunctions. In ICD-11 the group of sexual pain disorders contains Sexual pain-penetration disorder (HA20) and Dyspareunia (GA12). HA20 includes both the pain component and the spastic one (contraction of muscles that prevents penetration of the vagina). Factors of somatic / organic and nonsomatic / inorganic modality may participate in the appearance of this disorder. When comparing the above disorder with those, which reflect in ICD-10, we should note its partial correspondence with Nonorganic vaginismus – code F52.5, Nonorganic dyspareunia – code F52.6 and Vaginismus (organic) – code N94.2. Such a diagnosis as vaginismus is absent in ICD-11. Code GA12 (Dyspareunia) in ICD-11 implies only physical determinants of the disorder and corresponds with code N94.1 (Dyspareunia [organic]) in ICD-10.
Sources of the appearance of the diagnosis “Sexual pain-penetration disorder” (HA20) should be looked for in DSM-5, where the diagnosis “Genito-pelvic pain/penetration disorder” (code 302.76) exists. This case deals with a combined diagnosis, which unites vaginismus and dyspareunia. In this classification, the solution about the necessity to make such a generalized diagnosis has been taken with reference to the fact that both these disorders are highly comorbid and hard to distinguish. Despite difficulties in their differential diagnosis, in our clinical practice we nevertheless focus on their differentiation, although often they can exist jointly.
We have compiled a comparative table of codes for sexual dysfunctions and codes for sexual pain disorders in ICD-10 and ICD-11.
Table: Sexual dysfunctions and sexual pain disorders in ICD-10 and ICD-11.
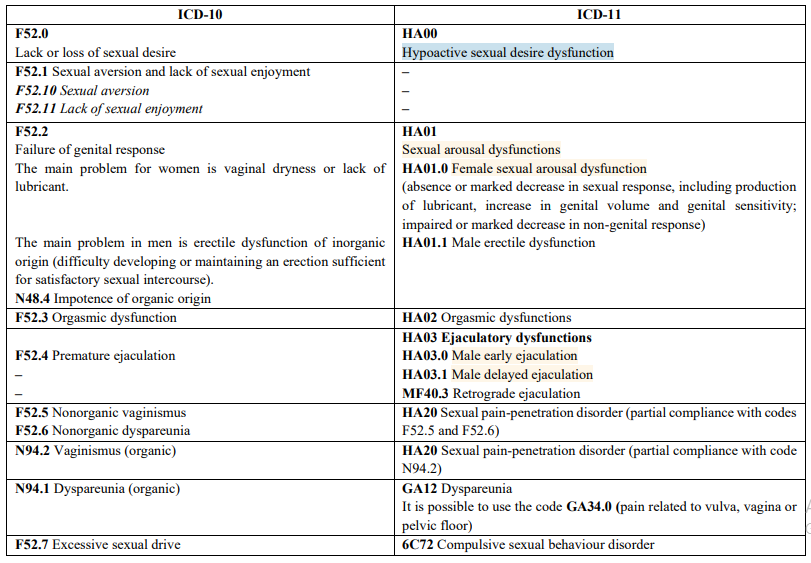
In the given table, we are talking about the partial correspondence of the code HA20 (ICD-11) to the codes F52.5, F52.6 and N94.2 (ICD-10), because in the characteristic of HA20 it is noted that this disorder is not fully explained by the factors of somatic modality.
As the WHO sought to distance itself from the rigid Cartesian separation of mind and body, which it considers outdated, organic and inorganic disorders were combined. Therefore, the section “Sexual dysfunctions not caused by organic diseases”, which previously existed in ICD-10, is absent in ICD-11. In this regard, the etiological aspects of sexual dysfunctions and sexual pain disorders (code HA40) are distinguished in ICD-11. This code is additionally added to the main code, which indicates an existing disorder, and, depending on the etiology, has subcodes HA40.1, HA40.2, HA40.3, HA40.4, HA40.5, HA40.Y.
In ICD-11 this diagnosis substituted for such ICD-10 diagnoses as transsexualism (F64.0) and gender identity disorders in children (F64.1). Transsexualism was called gender incongruence of adolescence and adulthood (HA60), and gender identity disorders in children were called gender incongruence of childhood (HA61). It should be emphasized that transsexualism was excluded from the list of mental disorders proceeding from social effects without any scientific grounds (Kocharyan, 2019). At present, Ukraine has not changed over to using ICD-11; hence, transsexualism and gender identity disorders in children are regarded as mental disorders.
In ICD-11 the chapter, which deals with gender incongruence, uses the concept “assigned sex”. Assigned sex or sex of parenting is the one, in belonging to which the child is brought up. As a rule, this sex coincides with the child’s sex and his/her passport sex, but not always. In the overwhelming majority of cases a child is brought up in that sex, which was identified by the obstetrician and/or legally recognized in documents. But sometimes upbringing may not comply with the child’s sex, because his/her parents wanted to have got a child of another sex. Also, the sex of parenting does not always coincide with the biological sex of the child, especially in cases of intersexuality or mistakes with sex identification at birth (Assigned sex, 2024).
In our opinion, the use of the word combination “assigned sex” gives a somewhat unusual meaning to this definition. Obviously, the term “established sex” or “established biological/anatomical sex” should be regarded as more appropriate in this case.
It should be noted that in ICD-10 the chapter of gender identity disorders also included such pathology as dual-role transvestism (code F64.1). This disorder is characterized by the fact that for a certain period of time a person dresses up in clothes of the opposite sex in order to enjoy temporary experience of being in that sex, but without any desire to change one’s own sex and undergo a surgical intervention related to it. Sexual excitement, which accompanies dressing up in clothes of the other sex, is absent. In ICD-11 the chapter, which deals with gender incongruence, does not contain the characterized disorder.
ICD-10 has chapter F66 (“Psychological and behavioural disorders associated with sexual development and orientation”), which describes such a situation when sexual identity or sexual preference do not provoke any doubt, but the individual wants that they were other because of additionally present mental or behavioural disorders and may look for treatment with aim to change them (The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines, 1992).
In 2014 the WHO appointed a group of ICD-11 developers, who recommended that the above chapter should be excluded from ICD. In the context that homosexual orientation in this classification is not regarded as pathology by itself, the wish to get rid of the above orientation, which in this case is called egodystonic and belongs to code F66.1 (“Egodystonic sexual orientation”), allegedly shows that there is some abnormality. It is reported that in order to exclude this chapter the developers were guided by the following assumption. Homosexual and bisexual people often feel a higher level of distress that is related to their social rejection and discrimination, and these individuals, as the above group believes, cannot be considered mentally sick. ICD-11, which was approved in 2019 and came into effect in January of 2022, does not contain any diagnostic categories that can apply to people on the basis of their sexual orientation (Egodystonic sexual orientation, 2024).
At the same time, it is necessary to cite the opinion of authoritative domestic sexologists (G. S. Vasilchenko, A. M. Svyadoshch, S. S. Libikh, V. V. Krishtal) and some famous foreign specialists, such as Joseph Nicolosi, who do not consider homosexuality a norm (Kocharyan, 2008). One of the main arguments in this case is the exclusion of homosexuals from the process of reproduction of the human race.
In ICD-11 sexual perversions are called paraphilic disorders, which in ICD-10 were termed as disorders of sexual preference (F65). Diagnostic criteria for research of ICD-10 define them as follows: typical for the individual are periodically appearing intense sexual urges and fantasies, which include unusual objects or acts (G1); the individual either acts according to these urges or feels a significant distress caused by them (G2); this preference is observed at least 6 months (G3). Significantly, names of each paraphilia in ICD-11 contain the word “disorder”, and restrictive criteria are introduced in characterizing such disorders. For example, exhibitionistic disorder (6D30) does not include exhibitionistic behaviour by mutual consent that takes place by agreement of another person or other people as well as socially approved forms of exhibitionism. Voyeuristic disorder (6D31) includes voyeuristic behaviour by mutual consent, which takes place by agreement of another person or other people, who are watched. Coercive sexual sadism disorder (6D33) excludes sexual sadism and masochism by mutual consent. Consequently, making of paraphilic actions by agreement transforms paraphilic disorder, which belongs to mental pathology, into paraphilia, which does not belong to the above pathology. Here we deal with an interesting situation, when the same person can be declared both mentally sick and mentally healthy. So, if a male sadist has sexual relations with a female masochist, he is declared mentally healthy. But as for the case, when he has sexual contacts with a woman, who does not have masochism and who does not accept sadistic behaviour from the side of the man, then he will be declared mentally sick. Besides, it is necessary to pay attention to the fact that in ICD-11 masochism is not listed among paraphilic disorders.
It is also necessary to pay attention to paedophilia (code F65.4 in ICD-10), which in ICD-11 is defined as pedophilic disorder (6D32). While in ICD-10 pedophilia includes sexual attraction to prepubertal and early pubertal children, in ICD-11 it includes only attraction to prepubertal persons. Consequently, in ICD-11 the age of children, to whom paedophils feel sexual urge, was decreased. In order to reveal more distinct age boundaries for objects of the sexual urge of paedophils it is reasonable to refer to DSM-5, which deals with children at the prepubertal age or the age of 13 or younger.
In general, as the presented material demonstrates, ICD-11 deals with partial depathologizing of sexual disorders that, in particular, has produced an effect on paraphilias (disorders of sexual preference).
Partial depathologizing of paraphilias can be also found in DSM-5 (Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition, 2013), where, for example, it is noted that if people inform about absence of feeling of guilt, shame or alarm caused by pedophilic impulses and are not functionally limited by them (according to self-reports, objective evaluations, etc.), while their self-reports and legally fixed data show that they have never acted following their impulses, then these people have pedophilic sexual orientation rather than pedophilic disorder. In light of the foregoing it is possible to say that the above case deals with a mental health norm (pedophilia) rather than mental pathology (pedophilic disorder).
In our opinion, partial depathologizing of paraphilias that was reflected in ICD-11 is from the medical point of view scientifically unsound, it results from effects of social factors only, and in making diagnoses of the above disorders it is reasonable to use the traditional approach to their definition.
Thus, the data presented in this article provide an opportunity for specialists in the field of sexual health to familiarize themselves with the innovations of ICD-11 related to various sexual disorders.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
