Assistant Vice President for Clinical Education Development, A.T. Still University Mesa, Arizona, United States.
*Corresponding Author: Leonard B. Goldstein, Assistant Vice President for Clinical Education Development, A.T. Still University Mesa, Arizona, United States.
Citation: Ethan Hopkins, William Nguyen, James F. Keane, Leonard B. Goldstein, (2025), Scoping Review of Prophylactic Treatments for Reducing Migraine Occurrences, Clinical Medical Reviews and Reports, 7(2); DOI:10.31579/2690-8794/255
Migraine is a prevalent neurological disorder with significant socioeconomic and quality-of-life burdens. While acute treatments exist, prophylactic therapies are essential to reducing monthly migraine days (MMDs). This scoping review evaluates pharmacologic, non-pharmacologic, and procedural interventions for migraine prevention, with an emphasis on osteopathic manipulative treatment (OMT), supplements, and emerging therapies.
Methods:
A comprehensive literature search was conducted across PubMed, ClinicalTrials.gov, Cochrane Library, OSTMED.Dr, Still OneSearch, CINAHL, ClinicalKey, and Scopus using standardized keywords. Grey literature sources, including major headache organizations, were also reviewed. Studies were included if they examined prophylactic migraine treatments and reported changes in MMDs.
Results:
Among pharmacologic interventions, onabotulinumtoxinA (Botox) and CGRP inhibitors demonstrated the greatest reductions in MMDs. Non-pharmacologic approaches, including OMT, acupuncture, and neuromodulation, showed varying effectiveness, often as adjunct therapies. Nutraceuticals, such as magnesium and riboflavin, provided modest benefits. Variability in study design, patient populations, and outcome measures impacted direct comparisons.
Conclusion:
A range of prophylactic treatments exist for reducing MMDs, with efficacy varying by patient population. While pharmacologic options remain primary, non-pharmacologic and procedural therapies offer promising alternatives. Future research should standardize outcome measures and explore personalized treatment approaches.
Introduction
Migraine is one of the most prevalent neurological disorders, and is a serious public health concern, affecting approximately 1 out of every 6 Americans. [1]. Although migraine is considered a benign disorder, the socioeconomic burden of migraine is substantial, with migraine-related lost productivity incurring extensive annual costs. [ -4]The clinical presentation of migraines is highly variable among individuals but commonly includes recurrent, intense unilateral throbbing headaches, often accompanied by anorexia, nausea, vomiting, phonophobia, and photophobia. [5-6] Acute migraine attacks are typically divided into four phases—prodrome, aura, headache, and postdrome—that follow a sequential progression. However, the specific manifestation, overlap, duration, and intensity of these phases can vary significantly between individuals and even across episodes. [7]The prodrome phase occurs hours to days before headache onset and is characterized by subtle warning signs like mood changes, neck stiffness, fatigue, increased urination and food cravings. [8] The aura phase, when present, manifests as transient neurological symptoms such as visual, sensory, or motor disturbances that typically develop within an hour of headache onset. [9] The headache phase is the most debilitating, marked by severe pain and sensitivity to external stimuli. Finally, the postdrome phase, often referred to as the "migraine hangover," is associated with lingering symptoms, including fatigue, difficulty concentrating, mood disturbances, and residual head discomfort.[10] Migraine attacks can be triggered by a variety of factors, including stress, illness, emotions, and hormonal fluctuations, such as those occurring during the menstrual cycle.Emerging research has advanced our understanding of migraine pathophysiology, shedding light on underlying mechanisms. Cortical spreading depression (CSD), a self-propagating wave of neuronal and glial depolarization across the cerebral cortex, has been implicated as a key driver of migraines. CSD is hypothesized to generate the aura phase, activate trigeminal nerve afferents, and disrupt the blood-brain barrier through matrix metalloproteinase activation and upregulation.[8] Additionally, while vasodilation of dural and extracranial vessels has long been considered central to migraine pain, recent findings challenge this theory, suggesting that other mechanisms may play a more pivotal role. [9]The pathophysiology of migraines involves the activation of the trigeminal vascular system. While vasodilation of cranial blood vessels is no longer considered the primary or sole mechanism behind migraines, our current understanding suggests that blood vessels still play a role. The reason for this logic is that blood vessels release and respond to various mediators, such as growth factors, cytokines, ATP, and NO, and many of these mediators are also known to have actions in neurons that can lead to migraines. On the other hand, blood vessels are capable of facilitating bi-directional communication with the nervous system through the release of substances like norepinephrine and calcitonin gene-related peptide (CGRP), which directly impact the cells present in the vessels. This means that various normal and pathological processes taking place within and among vascular cells can serve as channels for interaction between the vascular system and the nervous system, without requiring alterations in vascular tone. CGRP is a 37-amino acid neuropeptide that is produced as a consequence of alternative RNA processing of the calcitonin gene. It is known to have strong vasodilatory effects, and it is mainly released from C and Aδ sensory fibers. [] CGRP receptors are located in various neuronal tissues, such as the trigeminal ganglion, cerebral and meningeal vasculature, trigeminal nucleus caudalis (located in the brainstem) and the thalamus. Activation of these receptors within the trigeminovascular system plays an important role in the events that ultimately lead to the experience of pain with migraines, as evidenced by the ability of IV administered exogenous CGRP to cause migraine-like headaches. [ - ] After nerve stimulation, the release of CGRP occurs through calcium-dependent exocytosis from its storage vesicles. Once released, it is hypothesized that CGRP binds to CGRP receptors, and relays migraine pain through the brainstem into the brain via the trigeminovascular system. With this rather new discovery between the correlation of CGRP and migraines, many new studies have explored the efficacy of CGRP antagonists, specifically in comparison to other preventative medications. In fact, as of April 23, 2023, the FDA has approved expanding the indication of QULIPTA (atogepant) for the preventive treatment of migraine in adults. Atogepant has shown to significantly reduce monthly migraine days, monthly headache days, and monthly medication use days in comparison to a placebo, with no significant difference in adverse effects.While CGRP antagonists as well as other medication classes like the serotonin receptor agonists (triptans) have demonstrated efficacy in the acute treatment of migraines, the focus of this scoping review is distinct. This review aims to explore and evaluate a broad range of preventive interventions aimed at reducing the frequency of migraine attacks. These interventions include pharmacological agents, such as beta-blockers, antiepileptic drugs, and CGRP inhibitors, as well as non-pharmacological approaches, such as osteopathic manipulative treatment (OMT), acupuncture, and mindfulness-based therapies. Additionally, the review will assess the potential of nutraceuticals, including magnesium, riboflavin (vitamin B2), and coenzyme Q10, as well as dietary modifications and lifestyle interventions.The effectiveness of these preventive strategies will be evaluated based on their ability to reduce monthly migraine days (MMDs). It is important to note that this review will not focus on interventions aimed at decreasing the intensity or severity of migraine symptoms, which are often measured using tools such as the Headache Impact Test-6 (HIT-6) or the Migraine Disability Assessment (MIDAS) scores. By concentrating on MMD reduction, this review seeks to provide a targeted analysis of diverse approaches to migraine prevention, contributing to a deeper understanding of their roles in long-term management.
Methods
A comprehensive search strategy has been developed in consultation with a medical librarian (Leslie Golamb) to ensure breadth and relevance. The search began with an exploration of grey literature sources to refine keyword selection and identify additional relevant studies. Google was used for preliminary searches to explore osteopathic treatments for chronic migraines, uncover relevant grey literature, and establish key search terms. Information was gathered from reputable organizations, including the American Migraine Foundation, the Association of Migraine Disorders, the National Headache Foundation, and the American Academy of Neurology. These sources provided insights into current best practices, research priorities, and established approaches to migraine prophylaxis, helping to inform the direction of the database search.Following this preliminary investigation, systematic searches were conducted across multiple academic databases, including PubMed, ClinicalTrials.gov, Cochrane Library, OSTMED. Dr, Still One Search, CINAHL, Clinical Key, and Scopus. A standardized set of search terms was applied across databases to ensure consistency and comprehensive coverage. These included variations of "migraine," "migraine headache," "prophylactic treatment," "preventive treatment," "long-term treatment," "therapy," "intervention," "management," and "osteopathic manipulative treatment (OMT)." In PubMed, searches utilized Medical Subject Headings (MeSH) in combination with these keywords, while in other databases, similar Boolean strategies were employed to maximize relevant results. Filters were applied to restrict results to studies published from 2010 onward, with Scopus searches further refined to include only journal articles, conference proceedings, and trade journals from 2014 onward. ClinicalTrials.gov and the Cochrane Library were specifically searched for ongoing or completed clinical trials and systematic reviews evaluating OMT as a migraine prophylaxis. OSTMED. Dr, an osteopathic-focused database, was searched using the keyword “migraine headache.” Broad searches in Still One Search, CINAHL, and Clinical Key incorporated the same standardized terms, with filters applied for peer-reviewed journal articles. By maintaining consistency in search terminology, the review ensured a systematic and reproducible approach to identifying relevant literature.Our systematic search strategy ensured we captured a wide range of studies on prophylactic and preventive migraine treatments, with a specific emphasis on osteopathic interventions alongside supplements and medications. The inclusion criteria for this review were peer-reviewed articles published in English that addressed prophylactic treatments for chronic migraines, including pharmacological, non-pharmacological, or procedural interventions. Filters and date restrictions helped focus on the most recent and relevant research from 2010 onward. Studies that exclusively focused on acute treatment or did not provide evidence-based outcomes were excluded. This structured approach ensured a comprehensive review of existing evidence on prophylactic migraine treatments and their impact on reducing MMDs.
Figure 1:
* Reports were excluded at this stage if the study did not focus on either medications/ supplements/ or non-pharmacological modalities that can be used to prevent migraine occurrences
** Reports were excluded at this stage if the reduction in monthly migraine days was not explicitly reported or if the evidence quality was deemed insufficient
Reference: Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71.
Results
In our review, we included detailed information for each study, such as the population being studied, the intervention implemented, the outcomes measured, the study design, publication characteristics, quality of evidence, and the average reduction in monthly migraine days. Notably, all included articles provided a numerical value for the change in monthly migraine days, comparing the period before and after the intervention. However, it is important to highlight that several studies used the terms "migraine days" and "headache days" interchangeably, which may introduce variability in the reported outcomes.The evidence quality for each article in the chart is assessed using established research appraisal criteria frequently applied in evidence-based practice. Articles are classified into three categories: high, moderate, and low evidence quality. High-quality evidence includes randomized controlled trials (RCTs), systematic reviews, or meta-analyses with rigorous methodologies, adequate sample sizes, proper blinding and randomization, validated outcome measures, transparent and reproducible data, and publication in high-impact, peer-reviewed journals. Moderate-quality evidence encompasses cohort or observational studies and less robust systematic reviews, often with moderate sample sizes, limited blinding or randomization, and some methodological weaknesses, while still appearing in reputable peer-reviewed journals. Low-quality evidence involves case reports, case series, pilot studies, or poorly conducted observational studies, characterized by small sample sizes, lack of randomization or blinding, subjective outcome measures, and publication in lower-tier or non-peer-reviewed sources.Additionally, relevance to migraine prevention or treatment, disclosure of conflicts of interest, and publication recency are considered to ensure the evidence aligns with current clinical practices. These criteria provide a consistent and transparent framework for evaluating the quality of evidence included in the chart.
Data was then charted and organized first on evidence quality, then on the reduction of monthly migraine days.
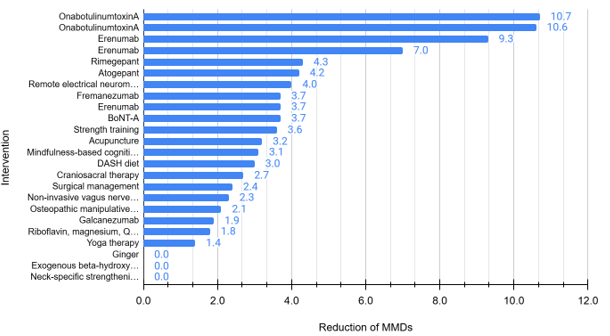
Figure 2: Chart of the included studies, looking at the intervention implemented in the study, and the mean reduction of monthly migraine days based on the intervention.
Discussion
Based on our review process and results, we were able to discover a wide variety of interventions implemented to decrease monthly migraine days in comparison to a placebo. Botox injections in patients with severe chronic migraines showed the greatest reduction of MMDs, with two studies reporting decreases of 10.7 and 10.6 days. Of the studies focused on onabotulinumtoxinA injections, the Phase III Research Evaluating Migraine Prophylaxis Therapy (PREEMPT) injection protocol was followed, which consists of injecting 155 U–195 U to 31–39 sites every 12-weeks.[1] The longevity between trials changed between studies, although the results of effectiveness were similar between trials and studies. However, it is important to note that in several studies, more than 10% of patients dropped out due to adverse side effects.
Erenumab, a calcitonin gene-related peptide (CGRP) monoclonal antibody, demonstrated moderate efficacy, with reductions in MMDs ranging from 7.0 to 9.3 days. The variation in effectiveness across studies suggests that while erenumab provides a meaningful reduction in migraine burden, the response may depend on patient characteristics and baseline migraine severity. Notably, one study reported that the confidence interval for MMD reduction overlapped with zero, indicating that some patients may not experience a significant benefit. This highlights the need for individualized treatment approaches and further research to identify which subgroups may respond best to erenumab.
Rimegepant, an oral CGRP receptor antagonist, showed a more modest reduction in MMDs, with a reported decrease of 4.3 days. While this reduction is smaller than that observed with Botox and erenumab, it is still clinically meaningful, particularly for patients with episodic migraines who may not require as aggressive prophylactic treatment. Given that rimegepant is an oral medication, it may offer a more convenient alternative to injectable treatments for some patients. However, the long-term effectiveness and adherence rates of rimegepant as a preventive option warrant further investigation.
Study Design and Evidence Quality
The included studies encompassed a range of methodological approaches, including randomized controlled trials (RCTs), systematic reviews, meta-analyses, and real-world observational studies. Each study was assessed for evidence quality based on established appraisal criteria, with all included studies classified as high-quality evidence. The incorporation of systematic reviews and meta-analyses strengthens the reliability of the findings, as these studies aggregate data from multiple sources to provide a more comprehensive assessment of treatment efficacy.
One notable strength of this review is the inclusion of long-term safety and subgroup analyses, which provide valuable insights into the sustained benefits and tolerability of migraine prophylactic treatments. While RCTs remain the gold standard for evaluating treatment efficacy, real-world data from observational studies and meta-analyses of clinical practice data add an important layer of external validity, reflecting how these treatments perform outside of controlled trial settings. However, differences in study design, patient populations, and treatment protocols introduce some heterogeneity, which must be considered when interpreting the findings.
Variability in Outcome Reporting
A major limitation identified in this review is the inconsistent use of terminology across studies, particularly regarding the distinction between migraine days (MMDs) and headache days (MHDs). While MMDs specifically refer to days with migraine-level headache symptoms, MHDs encompass a broader range of headache types, including tension-type headaches and less severe headache episodes. Some studies used these terms interchangeably, complicating direct comparisons. This inconsistency highlights the need for standardized outcome reporting in migraine research to enhance clarity and comparability across studies.
Studies reporting a substantial reduction in MMDs often demonstrated statistically significant outcomes. However, placebo groups in these trials also exhibited notable reductions in MMDs, emphasizing the potential impact of placebo effects. This underscores the importance of carefully interpreting the net treatment benefit while accounting for the active placebo response in migraine prophylaxis trials. For example, in the study by. on OnabotulinumtoxinA for migraine treatment, the placebo group experienced a 6.6-day reduction in MMDs compared to an 8.4-day reduction with Botox. Due to this significant placebo effect, the overall evidence quality was rated as “moderate” rather than “high,” highlighting the challenges in isolating true treatment effects in migraine prophylaxis research.
Additionally, variability in inclusion and exclusion criteria across the reviewed studies significantly affects result comparability. The baseline number of monthly migraine days (MMDs) varied widely, with some patient populations experiencing higher initial MMDs, making reductions appear more pronounced. These differences in study design and patient selection contribute to inconsistencies in treatment outcomes and reinforce the need for standardized baseline characteristics in migraine research to facilitate more reliable cross-study comparisons.
Clinical Implications
The findings of this review reinforce the clinical utility of prophylactic migraine treatments, particularly for patients with chronic migraines who experience frequent and debilitating attacks. The substantial reduction in MMDs with onabotulinumtoxinA and erenumab suggests that these treatments may be highly beneficial for patients with a high migraine burden. However, treatment selection should consider not only efficacy but also factors such as tolerability, adherence, and patient preference. For example, Botox requires in-office injections every 12 weeks, which may be inconvenient for some patients, whereas erenumab and rimegepant offer self-administered options with different dosing schedules.
In addition to pharmacologic interventions, non-pharmacologic approaches may also play a role in migraine prevention, either as standalone options for patients seeking alternatives or as adjunct therapies to enhance treatment outcomes. Acupuncture, osteopathic manipulative treatment (OMT), and exercise have shown some efficacy in reducing headache frequency and intensity, potentially providing relief with fewer side effects. Similarly, certain supplements, such as magnesium, riboflavin, and CoQ [10] have been associated with reductions in migraine frequency and may be especially appealing to patients who prefer lifestyle or dietary approaches.
Additionally, the findings highlight the importance of individualized treatment approaches, as some patients may respond better to certain interventions than others. Given the variability in response rates and the presence of adverse effects, shared decision-making between patients and healthcare providers is essential to optimize treatment outcomes. Future studies should explore biomarkers or predictive factors that can help identify which patients are most likely to benefit from specific prophylactic treatments, while also investigating the potential long-term benefits of incorporating non-pharmacologic options into comprehensive migraine management plans.
Limitations & Future Directions
While this review provides valuable insights into the effectiveness of prophylactic migraine treatments, several limitations should be acknowledged. Variability in study design, patient populations, and outcome reporting introduces challenges in directly comparing results across studies. The interchangeable use of migraine days and headache days highlights the need for greater standardization in migraine research methodologies.
Additionally, while RCTs provide high-quality evidence, real-world data on long-term adherence, effectiveness, and patient satisfaction are still limited. Future studies should focus on long-term observational studies and real-world registries to better understand treatment persistence and patient-reported outcomes. Furthermore, continued head-to-head trials comparing different prophylactic treatments will help refine clinical decision-making by directly assessing their relative efficacy, tolerability, and patient preference.
Conclusion
This scoping review underscores the effectiveness of onabotulinumtoxinA, erenumab, and rimegepant as prophylactic treatments for migraines, with Botox and CGRP inhibitors demonstrating the greatest reductions in MMDs. However, treatment tolerability, variability in response, and differences in outcome reporting highlight the need for an individualized approach to migraine prevention. Future research should prioritize long-term effectiveness, real-world adherence, and standardization of outcome measures to further guide evidence-based migraine management.
References
Adragna V, Bertino A, Carano M, Soru A, Taranto G, Desideri R (2015). O052. Migraine without aura and osteopathic medicine, a non-pharmacological approach to pain and quality of life: open pilot study...1st Joint ANIRCEF-SISC Congress. Rome, Italy. 29-31 October 2015. Journal of Headache & Pain. 16:1-3. View at Publisher |
View at Google Scholar
Al-Hadeethi RQ, Al-Ani. SK, Al-Ani RK (2020). Prevalence of Migraine Headache among Secondary School Students in Ramadi City, West of Iraq. Indian Journal of Public Health Research & Development;11(4):1584-1589. Accessed July 7, 2023. View at Publisher |
View at Google Scholar
Alexander J (2016). Resolution of New Daily Persistent Headache After Osteopathic Manipulative Treatment. J Am Osteopath Assoc;116(3):182-185. View at Publisher |
View at Google Scholar
Alsarhan H (2023). A scoring chart to evaluate cases of probable vestibular migraine. Hearing, Balance & Communication;21(3):162-168. View at Publisher |
View at Google Scholar
Arab A, Khorvash F, Kazemi M, Heidari Z, Askari G (2022). Effects of the Dietary Approaches to Stop Hypertension (DASH) diet on clinical, quality of life and mental health outcomes in women with migraine: a randomised controlled trial. British Journal of Nutrition. 128(8):1535-1544. View at Publisher |
View at Google Scholar
Argyriou AA, Dermitzakis EV, Vlachos GS, Vikelis M (2022). Long-term adherence, safety, and efficacy of repeated onabotulinumtoxinA over five years in chronic migraine prophylaxis. Acta Neurol Scand;145(6):676-683. View at Publisher |
View at Google Scholar
Armand CE, Loder E, Ropper AH (2022). Migraine - Treatment and Preventive Therapies. New England Journal of Medicine;387(15):e35. View at Publisher |
View at Google Scholar
Arnadottir TS, Sigurdardottir AK (2013). Is craniosacral therapy effective for migraine? Tested with HIT-6 Questionnaire. Complement Ther Clin Pract. 19(1):11-14. View at Publisher |
View at Google Scholar
Assarzadegan, Farhad; Asgarzadeh, Setareh; Hatamabadi, Hamid R.; Shahrami, Ali; Tabatabaey, Ali; et.al (2016). Serum concentration of magnesium as an independent risk factor in migraine attacks: a matched case–control study and review of the literature. International Clinical Psychopharmacology 31(5):p 287-292, September. View at Publisher |
View at Google Scholar
Badaeva AV, Danilov AB, Clayton P, et al (2023). Perspectives on Neuronutrition in Prevention and Treatment of Neurological Disorders. Nutrients. 15(11):2505. View at Publisher |
View at Google Scholar
Baldelli I, Mangialardi ML, Salgarello M, Raposio E (2020). Peripheral Occipital Nerve Decompression Surgery in Migraine Headache. Plastic and Reconstructive Surgery - Global Open;8(10):e3019. View at Publisher |
View at Google Scholar
Beier D, Callesen HE, Carlsen LN, et al (2022). Manual joint mobilisation techniques, supervised physical activity, psychological treatment, acupuncture and patient education in migraine treatment. A systematic review and meta-analysis. Cephalalgia;42(1):63-72. View at Publisher |
View at Google Scholar
Benatto MT, Florencio LL, Bragatto MM, Dach F, Fernández-de-las-Peñas C, Bevilaqua-Grossi D (2022). Neck-specific strengthening exercise compared with placebo sham ultrasound in patients with migraine: a randomized controlled trial. BMC Neurology;22(1):1-13. View at Publisher |
View at Google Scholar
Bennett MH, French C, Schnabel A, Wasiak J, Kranke P, Weibel S (2015). Normobaric and hyperbaric oxygen therapy for the treatment and prevention of migraine and cluster headache. Cochrane Database Syst Rev;2015(12):CD005219. Published 2015 Dec 28. View at Publisher |
View at Google Scholar
Biringer RG (2023). Migraine signaling pathways: purine metabolites that regulate migraine and predispose migraineurs to headache [published online ahead of print, 2023 Mar 22]. Mol Cell Biochem. 2023;10. View at Publisher |
View at Google Scholar
Bomtempo FF, Rocha RB, Cenci GI, Nager GB, Telles JPM (2023). Long-Term Safety and Effectiveness of Erenumab in Patients with Migraine: A Systematic Review and Single-Arm Meta-analysis. Clinical Drug Investigation;43(1):45-59. Accessed July 7, 2023. View at Publisher |
View at Google Scholar
Bond DS, Thomas JG, Lipton RB, et al (2018). Behavioral Weight Loss Intervention for Migraine: A Randomized Controlled Trial. Obesity (19307381). 2018;26(1):81-87. Accessed July 7, 2023. View at Publisher |
View at Google Scholar
Bronfort G, Assendelft WJ, Evans R, Haas M, Bouter L (2001). Efficacy of spinal manipulation for chronic headache: a systematic review. J Manipulative Physiol Ther. 24(7):457-466. View at Publisher |
View at Google Scholar
Bryson J, Buse DC, Lipton RB (2010). Assessment and treatment of the burden of migraine: a case series. Neurologist;16(4):254-261. View at Publisher |
View at Google Scholar
Buchanan EM, Manley HR, Sly JS, Cady RJ, Wikowsky A, Cunningham AL (2023). Development of the functional assessment of migraine scale using a patient guided approach. Quality of Life Research;32(3):867-879. View at Publisher |
View at Google Scholar
Burch R (2021). Preventive Migraine Treatment [published correction appears in Continuum (Minneap Minn). 2021 Oct 1;27(5):1494-1495]. Continuum (Minneap Minn). 2021;27(3):613-632. View at Publisher |
View at Google Scholar
Buse DC, Rabany L, Lin T, Ironi A, Connelly MA, Bickel JL (2022). Combining Guided Intervention of Education and Relaxation (GIER) with Remote Electrical Neuromodulation (REN) in the Acute Treatment of Migraine. Pain Medicine. 2022;23(9):1544-1549. View at Publisher |
View at Google Scholar
Carpenter A, Cardon B (2023). Transcutaneous electrical nerve stimulation decreases pain in acute migraine. Evidence-Based Practice. 2023;26(2):5. View at Publisher |
View at Google Scholar
Cassady B (2022). Spotlight on Supplements: Feverfew. Environmental Nutrition. 2022;45(10):3. Accessed July 11, 2023. View at Publisher |
View at Google Scholar
Cerritelli F, Emanuele C, Marcello DV, Luca M, Rina GL, Gabriella M (2013). Is osteopathic manipulative treatment effective in migraine? International Journal of Osteopathic Medicine;16(1):e15-6. View at Publisher |
View at Google Scholar
Cerritelli F, Ginevri L, Messi G, et al (2015). Clinical effectiveness of osteopathic treatment in chronic migraine: 3-Armed randomized controlled trial. Complement Ther Med;23(2):149-156. View at Publisher |
View at Google Scholar
Charles A (2018). A new opportunity after migraine treatment failure? Lancet (London, England);392(10161):2241-2242. View at Publisher |
View at Google Scholar
Channell MK, Mueller LL, Hahn R (2009). Management of chronic posttraumatic headache: a multidisciplinary approach. JAOA: Journal of the American Osteopathic Association;109(9):509-513. Accessed July 11, 2023. View at Publisher |
View at Google Scholar
Chenghui Pi, Yinglu Liu, Lingling Li, et al (2022). Effects on neuromodulation, acupuncture, and aerobic exercises on migraine and tension-type headache outcomes: A systematic review and meta-analysis. Medicine;101(45):1-13. View at Publisher |
View at Google Scholar
Christiansen S, Jürgens TP, Klinger R (2015). Outpatient Combined Group and Individual Cognitive-Behavioral Treatment for Patients With Migraine and Tension-Type Headache in a Routine Clinical Setting. Headache;55(8):1072-1091. View at Publisher |
View at Google Scholar
ClinicalTrials.gov. Comparison of Craniosacral therapy and Myofacial relaxation techniques in people diagnosed with migraine. View at Publisher |
View at Google Scholar
ClinicalTrials.gov. Osteopathic Manipulative Treatment and migraine headaches. https://classic.clinicaltrials.gov/ct2/show/NCT04976985 View at Publisher |
View at Google Scholar
Croop R, Lipton RB, Kudrow D, et al (2021). Oral rimegepant for preventive treatment of migraine: a phase 2/3, randomised, double-blind, placebo-controlled trial. Lancet. 397(10268):51-60. View at Publisher |
View at Google Scholar
Cuneo A, Yang R, Zhou H, et al (2023). The Utility of a Novel, Combined Biofeedback-Virtual Reality Device as Add-on Treatment for Chronic Migraine: A Randomized Pilot Study. Clinical Journal of Pain. 2023;39(6):286-296. View at Publisher |
View at Google Scholar
Derry CJ (2023). Sumatriptan (all routes of administration) for acute migraine attacks in adults ‐ overview of Cochrane reviews. Derry S, Moore RA, Derry S, eds. Cochrane Database of Systematic Reviews. (5). Accessed July 7, 2023. View at Publisher |
View at Google Scholar
Di Lorenzo C, Coppola G, Sirianni G, et al (2015). Migraine improvement during short lasting ketogenesis: a proof-of-concept study. Eur J Neurol;22(1):170-177. View at Publisher |
View at Google Scholar
Diaz K, Chowdhury S, Gegbe N (2018). Is ginger effective for migraine headaches? Evidence-Based Practice. 2018;21(7):E10. View at Publisher |
View at Google Scholar
Diener HC, Goadsby PJ, Ashina M, et al (2019). Non-invasive vagus nerve stimulation (nVNS) for the preventive treatment of episodic migraine: The multicentre, double-blind, randomised, sham-controlled PREMIUM trial. Cephalalgia. 2019;39(12):1475-1487. View at Publisher |
View at Google Scholar
D'Ippolito M, Tramontano M, Buzzi MG (2017). Effects of Osteopathic Manipulative Therapy on Pain and Mood Disorders in Patients With High-Frequency Migraine. J Am Osteopath Assoc;117(6):365-369. View at Publisher |
View at Google Scholar
D'Onofrio F, Raimo S, Spitaleri D, Casucci G, Bussone G (2017). Usefulness of nutraceuticals in migraine prophylaxis. Neurol Sci. 2017;38(Suppl 1):117-120. View at Publisher |
View at Google Scholar
Dominguez-Moreno R, Do TP, Ashina M (2022). Calcitonin gene-related peptide and pituitary adenylate cyclase-activating polypeptide in migraine treatment. Current opinion in endocrinology, diabetes, and obesity;29(2):225-231. View at Publisher |
View at Google Scholar
Donnet A, Ducros A, Radat F, Allaf B, Chouette I, Lanteri-Minet M (2021). Severe migraine and its control: A proposal for definitions and consequences for care. Rev Neurol (Paris);177(8):924-934. View at Publisher |
View at Google Scholar
Dougherty CO, Silberstein SD (2012). OnabotulinumtoxinA in the treatment of migraine headache. Techniques in Regional Anesthesia and Pain Management;16(1):41-46. View at Publisher |
View at Google Scholar
Dyńka D, Kowalcze K, Paziewska A (2022). The Role of Ketogenic Diet in the Treatment of Neurological Diseases. Nutrients;14(23):5003. View at Publisher |
View at Google Scholar
Eigenbrodt AK, Ashina H, Khan S, et al (2021). Diagnosis and management of migraine in ten steps. Nat Rev Neurol;17(8):501-514. View at Publisher |
View at Google Scholar
El-Hawary H, Kavanagh K, Janis JE (2023). The Positive and Negative Predictive Value of Targeted Diagnostic Botox Injection in Nerve Decompression Migraine Surgery. Plastic and Reconstructive Surgery. June 2023. View at Publisher |
View at Google Scholar
Esparham A, Stark-Inbar A, Jekel L, et al (2023). Acute Treatment of Migraine in Adolescents: Real-World Analysis of Remote Electrical Neuromodulation (REN). Pediatric Neurology.142:51-55. View at Publisher |
View at Google Scholar
Espí-López GV, Ruescas-Nicolau MA, Nova-Redondo C, Benítez-Martínez JC, Dugailly PM, Falla D (2018). Effect of Soft Tissue Techniques on Headache Impact, Disability, and Quality of Life in Migraine Sufferers: A Pilot Study. J Altern Complement Med. 2018;24(11):1099-1107. View at Publisher |
View at Google Scholar
Feng X-X, Huang K-Y, Chen L, Zhou K (2023). Clinical efficacy of the shallow puncture and more-twirling acupuncture method in migraine treatment and its effects on serum 5-HT and β -EP levels. Technology & Health Care;31:533-540. View at Publisher |
View at Google Scholar
Estave PM, Margol C, Beeghly S, et al (2023). Mechanisms of mindfulness in patients with migraine: Results of a qualitative study. Headache: The Journal of Head & Face Pain;63(3):390-409. View at Publisher |
View at Google Scholar
Ferracini GN, Florencio LL, Dach F, et al (2017). Myofascial Trigger Points and Migraine-related Disability in Women With Episodic and Chronic Migraine. Clin J Pain. 33(2):109-115. View at Publisher |
View at Google Scholar
Gaul C, Diener HC, Danesch U; Migravent® Study Group(2015). Improvement of migraine symptoms with a proprietary supplement containing riboflavin, magnesium and Q10: a randomized, placebo-controlled, double-blind, multicenter trial. J Headache Pain. 16:516. View at Publisher |
View at Google Scholar
Gertsch E, Loharuka S, Wolter-Warmerdam K, Tong S, Kempe A, Kedia S (2014). Intravenous magnesium as acute treatment for headaches: a pediatric case series. J Emerg Med;46(2):308-312. View at Publisher |
View at Google Scholar
Gfrerer L, Raposio E, Ortiz R, Austen WG (2018). Surgical Treatment of Migraine Headache: Back to the Future. Plastic and Reconstructive Surgery. 2018;142(4):1036-1045. View at Publisher |
View at Google Scholar
Goadsby PJ (2006). Migraine: emerging treatment options for preventive and acute attack therapy. Expert Opin Emerg Drugs;11(3):419-427. View at Publisher |
View at Google Scholar
Gross E, Putananickal N, Orsini AL, et al (2019). Efficacy and safety of exogenous ketone bodies for preventive treatment of migraine: A study protocol for a single-centred, randomised, placebo-controlled, double-blind crossover trial. Trials;20(1):61. Published 2019 Jan 17. View at Publisher |
View at Google Scholar
Guo W, Jin H, Wang Y, et al (2021). Efficacy and safety of cutting therapy in the treatment of migraine: A protocol for systematic review and meta-analysis. Medicine. 100(50):e28084. View at Publisher |
View at Google Scholar
Guy’s and St Thomas’ NHS Foundation Trust, King’s College Hospital NHS Trust. A Feasibility Clinical Trial to Evaluate High Frequency Spinal Cord Stimulation for the Treatment of Patients With Chronic Migraine (rCM HF-SCS). Accessed July 7, 2023. View at Publisher |
View at Google Scholar
Haller H, Lauche R, Sundberg T, Dobos G, Cramer H (2019). Craniosacral therapy for chronic pain: a systematic review and meta-analysis of randomized controlled trials. BMC Musculoskelet Disord;21(1):1. Published 2019 Dec 31. View at Publisher |
View at Google Scholar
He K, Zhan M, Li X, Wu L, Liang K, Ma R (2022). A Bibliometric of Trends on Acupuncture Research About Migraine: Quantitative and Qualitative Analyses. J Pain Res ;15:1257-1269. Published 2022 Apr 28. View at Publisher |
View at Google Scholar
Heineman K (2018). Osteopathic Manipulative Treatment in the Management of Pediatric Headache and Orthodontic Intervention: A Case Report. AAO Journal. 28(1):15-18. Accessed July 11, 2023. View at Publisher |
View at Google Scholar
Hsu Y, Chen C, Wu S, Chen K (2023). Cold intervention for relieving migraine symptoms: A systematic review and meta‐analysis. Journal of Clinical Nursing (John Wiley & Sons, Inc). 2023;32(11/12):2455-2465. View at Publisher |
View at Google Scholar
Igarashi H, Shibata M, Ozeki A, Matsumura T (2023). Galcanezumab Effects on Migraine Severity and Symptoms in Japanese Patients with Episodic Migraine: Secondary Analysis of a Phase 2 Randomized Trial. Neurology and Therapy12(1):73-87. View at Publisher |
View at Google Scholar
Ishiyama S, Shibata Y, Ayuzawa S, Matsushita A, Matsumura A, Ishikawa E(2022). Modifying of Functional Connectivity Induced by Peripheral Nerve Field Stimulation using Electroacupuncture for Migraine: A Prospective Clinical Study. Pain Medicine. 23(9):1560-1569. View at Publisher |
View at Google Scholar
Jafari M, Bahrpeyma F, Togha M, Vahabizad F, Hall T (2023). Effects of Upper Cervical Spine Manual Therapy on Central Sensitization and Disability in Subjects with Migraine and Neck Pain. Muscles, Ligaments & Tendons Journal (MLTJ). 2023;13(1):177-185. View at Publisher |
View at Google Scholar
Janis JE, Barker JC, Palettas M (2017). Targeted Peripheral Nerve-directed Onabotulinumtoxin A Injection for Effective Long-term Therapy for Migraine Headache. Plastic and Reconstructive Surgery - Global Open. 2017;5(3):e1270. View at Publisher |
View at Google Scholar
Jara Silva CE, Joseph AM, Khatib M, et al (2022). Osteopathic Manipulative Treatment and the Management of Headaches: A Scoping Review. Cureus. 14(8): e27830. Published 2022 Aug 9. View at Publisher |
View at Google Scholar
Jose A, Nagori SA, Roychoudhury A (2018). Surgical Management of Migraine Headache. Journal of Craniofacial Surgery. 29(2):e106-e108. View at Publisher |
View at Google Scholar
Kaar CRJ, Gerard JM, Nakanishi AK (2016). The Use of a Pediatric Migraine Practice Guideline in an Emergency Department Setting. Pediatric Emergency Care. 32(7):435-439. View at Publisher |
View at Google Scholar
Karlsson WK, Ashina H, Cullum CK, et al (2023). The Registry for Migraine (REFORM) study: methodology, demographics, and baseline clinical characteristics. J Headache Pain;24(1):70. Published 2023 Jun 12. View at Publisher |
View at Google Scholar
King HH (2017). Manual Craniosacral Therapy May Reduce Symptoms of Migraine Headache. J Am Osteopath Assoc;117(1):59. View at Publisher |
View at Google Scholar
Kirell A, Shingleton R (2018). Mobile Behavioral Therapy for Headache: Pilot Study. Journal of Medical Internet Research;20(9):28. View at Publisher |
View at Google Scholar
Kopel D, Gottschalk CH (2023). Migraine--Not Just a Numbers Game: Aim to Improve Quality of Life. Neurology. 2023;100(8):357-358. View at Publisher |
View at Google Scholar
Korucu O, Dagar S, Çorbacioglu ŞK, Emektar E, Cevik Y (2018). The effectiveness of greater occipital nerve blockade in treating acute migraine‐related headaches in emergency departments. Acta Neurologica Scandinavica;138(3):212-218. View at Publisher |
View at Google Scholar
Kovacevic G, Stevanovic D, Bogicevic D, et al (2017). A 6-month follow-up of disability, quality of life, and depressive and anxiety symptoms in pediatric migraine with magnesium prophylaxis. Magnes Res. 2017;30(4):133-141. View at Publisher |
View at Google Scholar
Lanteri-Minet M, Ducros A, Francois C, Olewinska E, Nikodem M, Dupont-Benjamin L (2022). Effectiveness of onabotulinumtoxinA (BOTOX®) for the preventive treatment of chronic migraine: A meta-analysis on 10 years of real-world data. Cephalalgia. 42(14):1543-1564. View at Publisher |
View at Google Scholar
Law EF, Ritterband L, Zhou C, Palermo TM (2023). Intervention for Sleep and Pain in Youth (ISPY-RCT): protocol for a two-phase randomized controlled trial of sequenced cognitive-behavioral therapy for insomnia and pain management in adolescents with migraine. Trials;24(1):1-14. View at Publisher |
View at Google Scholar
Law S, Derry S, Moore RA (2013). Naproxen with or without an antiemetic for acute migraine headaches in adults. Cochrane Database Syst Rev. 2013;2013(10):CD009455. Published 2013 Oct 20. View at Publisher |
View at Google Scholar
Li D, Guo Y, Xia M, Zhang J, Zang W (2022). Dietary intake of thiamine and riboflavin in relation to severe headache or migraine: A cross‐sectional survey. Headache: The Journal of Head & Face Pain;62(9):1133-1142. View at Publisher |
View at Google Scholar
Linde K, Allais G, Brinkhaus B, et al (2016). Acupuncture for the prevention of episodic migraine. Cochrane Database Syst Rev.2016(6):CD001218. Published 2016 Jun 28. View at Publisher |
View at Google Scholar
Lipton JA, Matthew E (2014). Resolution of post-traumatic temporomandibular joint pain, headache and vision changes with OMM in the unified field: A case report. American Academy of Osteopathy Journal;24(1):22-28. View at Publisher |
View at Google Scholar
Lipton RB, Croop R, Stock DA, et al (2023). Safety, tolerability, and efficacy of zavegepant 10 mg nasal spray for the acute treatment of migraine in the USA: a phase 3, double-blind, randomised, placebo-controlled multicentre trial. Lancet Neurology. 22(3):209-217. View at Publisher |
View at Google Scholar
Lipton RB, Pozo-Rosich P, Blumenfeld AM, et al (2023). Effect of Atogepant for Preventive Migraine Treatment on Patient-Reported Outcomes in the Randomized, Double-blind, Phase 3 ADVANCE Trial. Neurology;100(8):e764-e777. View at Publisher |
View at Google Scholar
Lipton RB, Silberstein SD (2015). Episodic and Chronic Migraine Headache: Breaking Down Barriers to Optimal Treatment and Prevention. Headache: The Journal of Head & Face Pain. 55:103-122. Accessed July 7, 2023. View at Publisher |
View at Google Scholar
Lipton RB, Silberstein S (2018). Migraine Headache: Diagnosis and Current and Emerging Preventive Treatments. Prim Care Companion CNS Disord. 2018;20 suppl E1:li17059su1c. Published 2018 Dec 27. View at Publisher |
View at Google Scholar
Loh NR, Whitehouse WP, Howells R (2022). What is new in migraine management in children and young people?. Arch Dis Child;107(12):1067-1072. View at Publisher |
View at Google Scholar
Long C, Ye J, Chen M, Gao D, Huang Q (2022). Effectiveness of yoga therapy for migraine treatment: A meta-analysis of randomized controlled studies. American Journal of Emergency Medicine;58:95-99. View at Publisher |
View at Google Scholar
Lucius K (2022). Migraine Headache: Dietary Approaches and Nutritional Supplements. Integrative & Complementary Therapies;28(2):93-103. View at Publisher |
View at Google Scholar
Lucia Mangialardi M, Baldelli I, Salgarello M, Raposio E (2020). Decompression Surgery for Frontal Migraine Headache. Plastic and Reconstructive Surgery - Global Open. 2020;8(10):e3084. View at Publisher |
View at Google Scholar
Ma P, Dong X, Qu Y, et al (2021). A Narrative Review of Neuroimaging Studies in Acupuncture for Migraine. Pain Research & Management. November 2021:1-9. View at Publisher |
View at Google Scholar
Maier JA, Pickering G, Giacomoni E, Cazzaniga A, Pellegrino P(2020). Headaches and Magnesium: Mechanisms, Bioavailability, Therapeutic Efficacy and Potential Advantage of Magnesium Pidolate. Nutrients. 2020;12(9):2660. View at Publisher |
View at Google Scholar
Mainnah M, Septriana M, M. S. W (2022). The Role of Acupuncture Therapy to Overcome Oneside Head Pain (Migraine). Journal of Vocational Health Studies. 5(3):192-202. View at Publisher |
View at Google Scholar
Mann JD, Faurot KR, Wilkinson L, et al (2008). Craniosacral therapy for migraine: protocol development for an exploratory controlled clinical trial. BMC Complement Altern Med ;8:28. Published 2008 Jun 9. View at Publisher |
View at Google Scholar
Mannix S, Skalicky A, Buse DC, et al (2016). Measuring the impact of migraine for evaluating outcomes of preventive treatments for migraine headaches. Health & Quality of Life Outcomes;14:1-11. View at Publisher |
View at Google Scholar
Martic-Biocina S, Zivoder I, Kozina G (2017). Biofeedback and neurofeedback application in the treatment of migraine. Psychiatr Danub. 2017;29(Suppl 3):575-577. View at Publisher |
View at Google Scholar
Martin BR, Seaman DR (2015). Dietary and Lifestyle Changes in the Treatment of a 23-Year-Old Female Patient With Migraine. Journal of Chiropractic Medicine;14(3):205-211. View at Publisher |
View at Google Scholar
Martins LB, Rodrigues AM dos S, Monteze NM, et al (2020). Double-blind placebo-controlled randomized clinical trial of ginger ( ) in the prophylactic treatment of migraine. Cephalalgia;40(1):88-95. View at Publisher |
View at Google Scholar
Martinelli D, Pocora MM, De Icco R, et al (2023). Searching for the Predictors of Response to BoNT-A in Migraine Using Machine Learning Approaches. Toxins (Basel). 15(6):364. Published 2023 May 29. View at Publisher |
View at Google Scholar
Matera DV, Smith B, Lam B (2019). Revisiting the expanded use of hyperbaric oxygen therapy for treatment of resistant migraines. Med Gas Res;9(4):238-240. View at Publisher |
View at Google Scholar
Meng SH, Wang MX, Kang LX, et al (2021). Dietary Intake of Calcium and Magnesium in Relation to Severe Headache or Migraine. Front Nutr. 2021; 8:653765. Published 2021 Mar 5. View at Publisher |
View at Google Scholar
Mitsikostas DD, Rapoport AM (2015). New players in the preventive treatment of migraine. BMC Med ;13:279. Published 2015 Nov 10. View at Publisher |
View at Google Scholar
Mo H, Chung SJ, Rozen TD, Cho SJ (2022). Oxygen Therapy in Cluster Headache, Migraine, and Other Headache Disorders. J Clin Neurol ;18(3):271-279. View at Publisher |
View at Google Scholar
Moisset X, Pereira B, Ciampi de Andrade D, Fontaine D, Lantéri-Minet M, Mawet J (2020). Neuromodulation techniques for acute and preventive migraine treatment: a systematic review and meta-analysis of randomized controlled trials. J Headache Pain. 21(1):142. Published 2020 Dec 10. View at Publisher |
View at Google Scholar
Moore JC, Miner JR (2012). Subcutaneous delivery of sumatriptan in the treatment of migraine and primary headache. Patient Preference & Adherence. 6:27-37. View at Publisher |
View at Google Scholar
Mouaanaki SA, Carlsen LN, Bendtsen L, Jensen RH, Schytz HW (2022). Treatment experiences and clinical characteristics in migraine and tension-type headache patients before the first visit to a tertiary headache center. Cephalalgia;42(11-12):1265-1273. View at Publisher |
View at Google Scholar
Movahed MR (2023). Highly Effective Pressure Point Applied Between the Thumb and Index Finger for the Treatment of Migraine Attacks. Alternative Therapies in Health & Medicine ;29(3):271-273. Accessed July 11, 2023. View at Publisher |
View at Google Scholar
Mueller LL (2007). Diagnosing and managing migraine headache. J Am Osteopath Assoc. 2007;107(10 Suppl 6):ES10-ES16. View at Publisher |
View at Google Scholar
Muñoz-Gómez E, Inglés M, Aguilar-Rodríguez M, et al (2022). Effect of a Craniosacral Therapy Protocol in People with Migraine: A Randomized Controlled Trial. J Clin Med;11(3):759. Published 2022 Jan 30. View at Publisher |
View at Google Scholar
Muñoz-Gómez E, Inglés M, Serra-Añó P, Espí-López GV (2021). Effectiveness of a manual therapy protocol based on articulatory techniques in migraine patients. A randomized controlled trial. Musculoskelet Sci Pract; 54:102386. View at Publisher |
View at Google Scholar
Muñoz-Gómez E, Serra-Añó P, Mollà-Casanova S, et al (2022). Potential Add-On Effects of Manual Therapy Techniques in Migraine Patients: A Randomised Controlled Trial. J Clin Med. 2022;11(16):4686. Published 2022 Aug 11. View at Publisher |
View at Google Scholar
Murray K, O’Neal KS, Weisz M (2015). Dietary suggestions for migraine preventions. American Journal of Health-System Pharmacy ;72(7):519-521. View at Publisher |
View at Google Scholar
Nagori SA, Jose A, Roychoudhury A (2019). Surgical Management of Migraine Headaches: A Systematic Review and Meta-analysis. Annals of Plastic Surgery. 83(2):232-240. View at Publisher |
View at Google Scholar
Natbony LR, Zhang N (2020). Acupuncture for Migraine: a Review of the Data and Clinical Insights. Curr Pain Headache Rep;24(7):32. Published 2020 May 29. View at Publisher |
View at Google Scholar
Nattagh-Eshtivani E, Sani MA, Dahri M, et al (2018). The role of nutrients in the pathogenesis and treatment of migraine headaches: Review. Biomed Pharmacother. 2018;102:317-325. View at Publisher |
View at Google Scholar
Nierenburg H, Stark-Inbar A (2022). Nerivio® remote electrical neuromodulation for acute treatment of chronic migraine. Pain Management;12(3):267-281. View at Publisher |
View at Google Scholar
Nierenburg H, Vieira JR, Lev N, et al (2020). Remote Electrical Neuromodulation for the Acute Treatment of Migraine in Patients with Chronic Migraine: An Open-Label Pilot Study. Pain and Therapy ;9(2):531-543. View at Publisher |
View at Google Scholar
A non‐oral gepant for acute treatment of migraine. Headache: The Journal of Head & Face Pain. 2022;62(9):1075-1076. View at Publisher |
View at Google Scholar
Odawara M, Hashizume M, Yoshiuchi K, Tsuboi K (2015). Real-Time Assessment of the Effect of Biofeedback Therapy with Migraine: A Pilot Study. Int J Behav Med;22(6):748-754. View at Publisher |
View at Google Scholar
Ohlsen BA (2012). Combination of acupuncture and spinal manipulative therapy: management of a 32-year-old patient with chronic tension-type headache and migraine. Journal of Chiropractic Medicine11(3):192-201. View at Publisher |
View at Google Scholar
Ökmen BM, Güneş A, Altan L (2022). Evaluation of the efficacy of therapeutic ultrasound in the treatment of migraine. Turkish Journal of Physical Medicine & Rehabilitation (2587-1250);68(4):475-483. View at Publisher |
View at Google Scholar
Olesiejuk M, Marusiak J, Chalimoniuk M (2023). Myofascial Trigger Points therapy decreases myotonometric tone and stiffness of trapezius muscle, benefits headaches and muscle pain in migraine. NeuroRehabilitation;52(2):299-310. View at Publisher |
View at Google Scholar
Orr SL, Venkateswaran S (2014). Nutraceuticals in the prophylaxis of pediatric migraine: Evidence-based review and recommendations. Cephalalgia ;34(8):568-583. View at Publisher |
View at Google Scholar
Özge A, Uludüz D, Karadaş Ö, Mehtar Bozkurt M (2021). Erenumab in Mechanism-based Migraine Treatment. Turkish Journal of Neurology / Turk Noroloji Dergisi.;17(3):229-239. View at Publisher |
View at Google Scholar
Paemeleire K, Goodman AM (2012). Results of a patient survey for an implantable neurostimulator to treat migraine headaches. The Journal of Headache and Pain. 2012;13(3):239-241. View at Publisher |
View at Google Scholar
Pan L-LH, Chen W-T, Wang Y-F, et al (2022). Resting-state occipital alpha power is associated with treatment outcome in patients with chronic migraine. PAIN.163(7):1324-1334. View at Publisher |
View at Google Scholar
Pan L-LH, Hsiao F-J, Chen W-T, Wang S-J (2022). Resting State Electrophysiological Cortical Activity: A Brain Signature Candidate for Patients with Migraine. Current Pain and Headache Reports;26(4):289-297. View at Publisher |
View at Google Scholar
Parlongue G, Cerdan EV, Koenig J, Williams DP (2021). Smartphone based music intervention in the treatment of episodic migraine headaches – A pilot trial. Complementary Therapies in Medicine. 2021;63. View at Publisher |
View at Google Scholar
Patel PS, Minen MT (2019). Complementary and Integrative Health Treatments for Migraine. J Neuroophthalmol. 2019;39(3):360-369. View at Publisher |
View at Google Scholar
Peters GL, Hennessey EK (2021). Rimegepant: acute treatment for migraine headaches. Pain Management. 11(3):259-266. View at Publisher |
View at Google Scholar
Pietrzak D, Kasperek K, Rękawek P, Piątkowska-Chmiel I (2022). The Therapeutic Role of Ketogenic Diet in Neurological Disorders. Nutrients. 2022;14(9):1952. View at Publisher |
View at Google Scholar
Pires RD, Rocha NS, Esteves JE, Rodrigues ME (2017). Use of pressure dynamometer in the assessment of the pressure pain threshold in trigger points in the cranicervical muscles in women with unilateral migraine and tension-type headache: an observational study. International Journal of Osteopathic Medicine;26:28-35. View at Publisher |
View at Google Scholar
Plank S, Goodard JL, Pasierb L, Simunich TJ, Croner JR (2013). Standardized set-point acupuncture for migraines. Alternative Therapies in Health & Medicine;19(6):32-37. Accessed July 7, 2023. View at Publisher |
View at Google Scholar
Poudel S, Quinonez J, Choudhari J, et al (2021). Medical Cannabis, Headaches, and Migraines: A Review of the Current Literature. Cureus;13(8):e17407. Published 2021 Aug 24. View at Publisher |
View at Google Scholar
Puledda F, Goadsby PJ (2017). An Update on Non-Pharmacological Neuromodulation for the Acute and Preventive Treatment of Migraine. Headache. 2017;57(4):685-691. View at Publisher |
View at Google Scholar
Putananickal N, Gross EC, Orsini AL, et al (2022). Efficacy and safety of exogenous beta-hydroxybutyrate for preventive treatment in episodic migraine: A single-centred, randomised, placebo-controlled, double-blind crossover trial. Cephalalgia;42(4-5):302-311. View at Publisher |
View at Google Scholar
Rafie, Shahram & Namjoyan, Forough & Golfakhrabadi, Fereshteh & Yousefbeyk, Fatemeh & Hassanzadeh, Alireza(2016). Effect of lavender essential oil as a prophylactic therapy for migraine: A randomized controlled clinical trial. Journal of Herbal Medicine. 6. View at Publisher |
View at Google Scholar
Rajapakse T, Pringsheim T(2016). Nutraceuticals in Migraine: A Summary of Existing Guidelines for Use. Headache;56(4):808-816. View at Publisher |
View at Google Scholar
Rapoport AM, Freitag F, Pearlman SH (2010). Innovative delivery systems for migraine: The clinical utility of a transdermal patch for the acute treatment of migraine. CNS Drugs. 24(11):929-940. View at Publisher |
View at Google Scholar
Rezaeian T, Ahmadi M, Mosallanezhad Z, Nourbakhsh MR (2021). The impact of myofascial release and stretching techniques on the clinical outcomes of migraine headache: A randomized controlled trial. J Res Med Sci ; 26:45. Published 2021 Jul 31. View at Publisher |
View at Google Scholar
Rhyne DN, Anderson SL, Gedde M, Borgelt LM (2016). Effects of Medical Marijuana on Migraine Headache Frequency in an Adult Population. Pharmacotherapy. 36(5):505-510. View at Publisher |
View at Google Scholar
Rist PM, Hernandez A, Bernstein C, et al (2019). The Impact of Spinal Manipulation on Migraine Pain and Disability: A Systematic Review and Meta-Analysis. Headache. 59(4):532-542. View at Publisher |
View at Google Scholar
Rao R, Hershey AD (2020). An update on acute and preventive treatments for migraine in children and adolescents. Expert Rev Neurother ;20(10):1017-1027. View at Publisher |
View at Google Scholar
Rowlands E, Pozun A (2023). Osteopathic Manipulative Treatment: Suboccipital Release. In: StatPearls. Treasure Island (FL): StatPearls Publishing; March 8. View at Publisher |
View at Google Scholar
Rundblad L, Cullum CK, Sacco S, et al (2022). Use of Non-pharmacological Therapies in Individuals With Migraine Eligible for Treatment With Monoclonal Antibodies Targeting Calcitonin Gene-Related Peptide (CGRP)-Signaling: A Single-Center Cross-Sectional Observational Study. Front Pain Res (Lausanne). 2022;3:935183. View at Publisher |
View at Google Scholar
Safonov MI, Naprienko MV (2017). Analiz éffektivnosti refleksoterapii v kompleksnom lechenii khronicheskoĭ migreni [Analysis of the efficacy of reflexology in the complex treatment of chronic migraine]. Zh Nevrol Psikhiatr Im S S Korsakova;117(5):22-25. View at Publisher |
View at Google Scholar
Saigle V (2023). A patient’s perspective on trying to access migraine treatment in Northern British Columbia. CMAJ : Canadian Medical Association journal = journal de l’Association medicale canadienne;195(5):E198. View at Publisher |
View at Google Scholar
Saltychev M, Juhola J (2022). Effectiveness of High-Frequency Repetitive Transcranial Magnetic Stimulation in Migraine: A Systematic Review and Meta-analysis. American Journal of Physical Medicine & Rehabilitation. 2022;101(11):1001-1006. View at Publisher |
View at Google Scholar
Schwedt TJ (2019). New and Emerging Treatments for the Acute and Preventive Therapy of Migraine and Other Headaches. Headache ;59 Suppl 2:1-2. View at Publisher |
View at Google Scholar
Seddik AH, Schiener C, Ostwald DA, Schramm S, Huels J, Katsarava Z (2021). Social Impact of Prophylactic Migraine Treatments in Germany: A State-Transition and Open Cohort Approach. Value in Health;24(10):1446-1453. View at Publisher |
View at Google Scholar
Seng EK, Lipton RB (2022). Do behavioral treatments work for migraine prevention? Headache: The Journal of Head & Face Pain. 62(4):402-404. View at Publisher |
View at Google Scholar
Shauly O, Gould DJ, Sahai-Srivastava S, Patel KM (2019). Greater Occipital Nerve Block for the Treatment of Chronic Migraine Headaches: A Systematic Review and Meta-Analysis. Plastic and Reconstructive Surgery. 144(4):943-952. View at Publisher |
View at Google Scholar
Shoeibi A, Olfati N, Soltani Sabi M, Salehi M, Mali S, Akbari Oryani M (2017). Effectiveness of coenzyme Q10 in prophylactic treatment of migraine headache: an open-label, add-on, controlled trial. Acta Neurol Belg;117(1):103-109. View at Publisher |
View at Google Scholar
Silva ML, Martins LB, dos Santos LC, et al (2023). Decreased plasma levels and dietary intake of minerals in women with migraine. Nutritional Neuroscience. 2023;26(7):629-636. View at Publisher |
View at Google Scholar
Simshäuser K, Pohl R, Behrens P, Schultz C, Lahmann C, Schmidt S (2022). Mindfulness-Based Cognitive Therapy as Migraine Intervention: a Randomized Waitlist Controlled Trial. International Journal of Behavioral Medicine;29(5):597-609. View at Publisher |
View at Google Scholar
Slomski A (2022). Monoclonal Antibody Overcomes Migraine Treatment Failure. JAMA: Journal of the American Medical Association;328(8):700. View at Publisher |
View at Google Scholar
Smith MS, Olivas J, Smith K (2019). Manipulative Therapies: What Works. American Family Physician ;99(4):248-252. Accessed July 11, 2023. View at Publisher |
View at Google Scholar
Soleimanian-Boroujeni F, Badihian N, Badihian S, Shaygannejad V, Gorji Y (2023). The efficacy of transdiagnostic cognitive behavioral therapy on migraine headache: a pilot, feasibility study. BMC Neurology ;22(1):1-13. View at Publisher |
View at Google Scholar
Sorrel M (2010). Myofasical examination leads to diagnosis and successful treatment of migraine headache. Journal of Musculoskeletal Pain.18(1): 31-37. View at Publisher |
View at Google Scholar
Stern JI, Chiang C, Kissoon NR, Robertson CE (2022). Narrative review of peripheral nerve blocks for the management of headache. Headache: The Journal of Head & Face Pain;62(9):1077-1092. View at Publisher |
View at Google Scholar
Sun-Edelstein C, Mauskop A (2011).Alternative headache treatments: Nutraceuticals, behavioral and physical treatments. Headache ;51(3):469-483. View at Publisher |
View at Google Scholar
Sun-Edelstein C, Mauskop A (2009). Foods and supplements in the management of migraine headaches. Clin J Pain ;25(5):446-452. View at Publisher |
View at Google Scholar
Tepper SJ, Dodick DW, Schmidt PC, Kellerman DJ (2019). Efficacy of ADAM Zolmitriptan for the Acute Treatment of Difficult‐to‐Treat Migraine Headaches. Headache: The Journal of Head & Face Pain;59(4):509-517. View at Publisher |
View at Google Scholar
Tepper SJ, Grosberg B, Daniel O, et al (2022). Migraine treatment with external concurrent occipital and trigeminal neurostimulation—A randomized controlled trial. Headache: The Journal of Head & Face Pain. 2022;62(8):989-1001. View at Publisher |
View at Google Scholar
Tepper SJ, Lipton RB, Silberstein SD, et al (2023). Long-term efficacy and safety of erenumab in patients with chronic migraine and acute medication overuse: A subgroup analysis. Headache;63(6):730-742. View at Publisher |
View at Google Scholar
Tepper SJ, Rabany L, Cowan RP, et al (2023). Remote electrical neuromodulation for migraine prevention: A double‐blind, randomized, placebo‐controlled clinical trial. Headache: The Journal of Head & Face Pain;63(3):377-389. View at Publisher |
View at Google Scholar
Teubert JD, Courtney WD, Holeman RD, Kennedy CD (2020). Is osteopathic manipulative therapy as effective as medications for the treatment of headaches? Evidence-Based Practice;23(4):15-16. View at Publisher |
View at Google Scholar
Toprak Celenay S, Coban O, Mete O, Karahan N (2023). An investigation of the effects of connective tissue massage in women with migraine: A controlled clinical trial. Journal of Bodywork & Movement Therapies ;33:112-119. View at Publisher |
View at Google Scholar
Torabi R, Bourn L, Veith J, et al (2020). Population-Based Health Utility Assessment of Migraine Headache Symptoms before and after Surgical Intervention. Plastic and Reconstructive Surgery;145(1):210-217. View at Publisher |
View at Google Scholar
Torrisi M, Corallo F, Lo Buono V, et al (2023). Migraine Treatment Using Erenumab: Can Lead to a Cognitive and Psychological Qualitative Improvement?. Medicina (Kaunas);59(5):936. Published 2023 May 12. View at Publisher |
View at Google Scholar
Tiwari R, Tiwari G, Mishra S, Ramachandran V (2023). Preventive and Therapeutic Aspects of Migraine for Patient Care: An Insight. Curr Mol Pharmacol;16(2):147-160. View at Publisher |
View at Google Scholar
Tsung-Hsing Lin, Cheng-Chia Yang, Shih-Yu Lee, et al (2023). The effect of bright light therapy in migraine patients with sleep disturbance: A prospective, observational cohort study protocol. Frontiers in Aging Neuroscience; 15:1-6. View at Publisher |
View at Google Scholar
Tzankova V, Becker WJ, Chan TLH (2023). Diagnosis and acute management of migraine. Canadian Medical Association Journal (CMAJ) ;195(4):E153-E158. View at Publisher |
View at Google Scholar
Using osteopathy to treat musculoskeletal headaches and migraine. Indian Practitioner. 75(5):50. Accessed July 11, 2023. View at Publisher |
View at Google Scholar
Velásquez RV, Chachaima MJ, Cárdenas BEC, et al (2022). Greater occipital nerve block for chronic migraine patients: A meta‐analysis. Acta Neurologica Scandinavica. 146(2):101-114. View at Publisher |
View at Google Scholar
Visser EJ, Drummond PD, Lee-Visser JLA (2020). Reduction in Migraine and Headache Frequency and Intensity With Combined Antioxidant Prophylaxis (N-acetylcysteine, Vitamin E, and Vitamin C): A Randomized Sham-Controlled Pilot Study. Pain Pract. 20(7):737-747. View at Publisher |
View at Google Scholar
Voigt K, Liebnitzky J, Burmeister U, et al (2011). Efficacy of osteopathic manipulative treatment of female patients with migraine: results of a randomized controlled trial. J Altern Complement Med;17(3):225-230. View at Publisher |
View at Google Scholar
Walker D, Zhang N, Natbony LR (2023). Insomnia and Migraine: A Review of Evidence-Based, Biobehavioral Interventions. Current Pain & Headache Reports,27(2):19-25. View at Publisher |
View at Google Scholar
Whalen, J., Yao, S. & Leder, A (2018). A Short Review of the Treatment of Headaches Using Osteopathic Manipulative Treatment. Curr Pain Headache Rep 22, 82 (2018). View at Publisher |
View at Google Scholar
Winner PK, Blumenfeld AM, Eross EJ, et al (2019). Long-Term Safety and Tolerability of OnabotulinumtoxinA Treatment in Patients with Chronic Migraine: Results of the COMPEL Study. Drug Saf ;42(8):1013-1024. View at Publisher |
View at Google Scholar
Woldeamanuel YW, Oliveira ABD (2022). What is the efficacy of aerobic exercise versus strength training in the treatment of migraine? A systematic review and network meta-analysis of clinical trials. Journal of Headache & Pain.23(1):1-12. View at Publisher |
View at Google Scholar
Wu Q, Liu P, Liao C, Tan L (2022). Effectiveness of yoga therapy for migraine: A meta-analysis of randomized controlled studies. Journal of clinical neuroscience: official journal of the Neurosurgical Society of Australasia ;99:147-151. View at Publisher |
View at Google Scholar
Yan BM, Gibson Depoy EM, Ahmad A, Nahas SJ (2021). Biomarkers in Migraine. Neurology India;69(Supplement):S17-S24. View at Publisher |
View at Google Scholar
Yarnitsky D, Dodick DW, Grosberg BM, et al (2019). Remote Electrical Neuromodulation (REN) Relieves Acute Migraine: A Randomized, Double‐Blind, Placebo‐Controlled, Multicenter Trial. Headache: The Journal of Head & Face Pain;59(8):1240-1252. Accessed July 7, 2023. View at Publisher |
View at Google Scholar
Young N, Silverman D, Bradford H, Finkelstein J (2017). Multicenter prevalence of opioid medication use as abortive therapy in the ED treatment of migraine headaches. American Journal of Emergency Medicine.35(12):1845-1849. View at Publisher |
View at Google Scholar
Zhang Y, Dennis JA, Leach MJ, et al (2017). Complementary and Alternative Medicine Use Among US Adults With Headache or Migraine: Results from the 2012 National Health Interview Survey. Headache;57(8):1228-1242. View at Publisher |
View at Google Scholar
Zhao L, Chen J, Li Y, et al (2017). The Long-term Effect of Acupuncture for Migraine Prophylaxis: A Randomized Clinical Trial. JAMA Intern Med. 2017;177(4):508-515. View at Publisher |
View at Google Scholar
Zheng H, Fan S-Q, Shi Y-Z, Liang J-T, Xiao X-Y (2023). Matching adjusted indirect comparison of acupuncture versus fremanezumab in the preventive treatment of episodic migraine. Current Medical Research & Opinion. 2023;39(3):409-416. View at Publisher |
View at Google Scholar
Dear Jessica, and the super professional team of the ‘Clinical Cardiology and Cardiovascular Interventions’
I am sincerely grateful to the coordinated work of the journal team for the no problem with the submission of my manuscript: “Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report).”
The review process by 5 experts was fast, and the comments were professional, which made it more specific and academic, and the process of publication and presentation of the article was excellent.
I recommend that my colleagues publish articles in this journal, and I am interested in further scientific cooperation.
Sincerely and best wishes,
Dr. Oleg Golyanovskiy.
Dr Oleg Golyanovski
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.
Virginia E. Koenig
Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases.
Thank you for all.
Delcio G Silva Junior
Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article.
Specially thank you for the peer review process, support from the editorial office.
I appreciate positively the quality of your journal.
Ziemlé Clément Méda
Journal of Clinical Research and Reports
I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office.
The reviewer board were accurate and helpful regarding any modifications for my manuscript.
And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help.
It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.
Mina Sherif Soliman Georgy
We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work.
Hope for a more scientific relationship with your Journal.
Layla Shojaie
The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.
Sing-yung Wu
Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.
Orlando Villarreal
Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.
Katarzyna Byczkowska
Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.
Anthony Kodzo-Grey Venyo
Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.
Pedro Marques Gomes
Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.
Bernard Terkimbi Utoo
This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.
Prof Sherif W Mansour
Dear Hao Jiang, to Journal of Nutrition and Food Processing
We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.
Hao Jiang
As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal.
The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage.
The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful.
The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders.
In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dr Shiming Tang
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery,
Editorial Coordinator,
I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office.
The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.
Raed Mualem
International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.
Andreas Filippaios
Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity.
The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.
Dr Suramya Dhamija
Dear Erica Kelsey,
Editorial Coordinator of Cancer Research and Cellular Therapeutics
Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications.
We appreciated the very short time between the submission of the paper and its publication on line on your site.
Bruno Chauffert
I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article.
Have a good day!
Baheci Selen
"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".
Jesus Simal-Gandara
I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far.
Keep up the great work.
Douglas Miyazaki
We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.
Dr Griffith
I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.
Dr Tong Ming Liu
I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.
Husain Taha Radhi
I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery.
The peer review process, support from the editorial office, and quality of the journal are excellent.
The manuscripts published are of high quality and of excellent scientific value.
I recommend this journal very much to colleagues.
S Munshi
Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.
Tania Munoz
“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.
George Varvatsoulias
Dear editorial department:
On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal.
Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner.
I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality.
Sincerely,
Rui Tao.
Rui Tao
Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
Khurram Arshad
Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.
Gomez Barriga Maria Dolores
The peer reviewers process is quick and effective, the supports from editorial office is excellent,
the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.
Lin Shaw Chin
Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project.
I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality.
We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.
Maria Dolores Gomez Barriga
Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions,
I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients."
I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.
Dr Maria Dolores Gomez Barriga
Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing.
¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.
Dr Maria Regina Penchyna Nieto
Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions,
The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed.
The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.
Dr Marcelo Flavio Gomes Jardim Filho
Dear Editorial Coordinator of the Journal of Nutrition and Food Processing!
"I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”
Zsuzsanna Bene
Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner
Dr Susan Weiner
My Testimonial Covering as fellowing: Lin-Show Chin.
The peer reviewers process is quick and effective, the supports from editorial office is excellent,
the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.
Lin-Show Chin
My experience publishing in Psychology and Mental Health Care was exceptional.
The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work.
The editorial team was highly supportive and responsive, making the submission process smooth and efficient.
The journal's commitment to high standards and academic rigor makes it a respected platform for quality research.
I am grateful for the opportunity to publish in such a reputable journal.
Sonila Qirko
My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional.
I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
Luiz Sellmann
I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.
Zhao Jia
Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery,
"The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."
Thomas Urban
I would like to express my sincere gratitude for the support and efficiency provided by the editorial office throughout the publication process of my article, “Delayed Vulvar Metastases from Rectal Carcinoma: A Case Report.” I greatly appreciate the assistance and guidance I received from your team, which made the entire process smooth and efficient.
The peer review process was thorough and constructive, contributing to the overall quality of the final article. I am very grateful for the high level of professionalism and commitment shown by the editorial staff, and I look forward to maintaining a long-term collaboration with the International Journal of Clinical Case Reports and Reviews.
Cristina Berriozabal
To Dear Erin Aust,
I would like to express my heartfelt appreciation for the opportunity to have my work published in this esteemed journal. The entire publication process was smooth and well-organized, and I am extremely satisfied with the final result. The Editorial Team demonstrated the utmost professionalism, providing prompt and insightful feedback throughout the review process. Their clear communication and constructive suggestions were invaluable in enhancing my manuscript, and their meticulous attention to detail and dedication to quality are truly commendable.
Additionally, the support from the Editorial Office was exceptional. From the initial submission to the final publication, I was guided through every step of the process with great care and professionalism. The team's responsiveness and assistance made the entire experience both easy and stress-free.
I am also deeply impressed by the quality and reputation of the journal. It is an honor to have my research featured in such a respected publication, and I am confident that it will make a meaningful contribution to the field.
Dr Tewodros Kassahun Tarekegn
"I am grateful for the opportunity of contributing to [International Journal of Clinical Case Reports and Reviews] and for the rigorous review process that enhances the quality of research published in your esteemed journal. I sincerely appreciate the time and effort of your team who have dedicatedly helped me in improvising changes and modifying my manuscript. The insightful comments and constructive feedback provided have been invaluable in refining and strengthening my work".
Dr Shweta Tiwari
I thank the ‘Journal of Clinical Research and Reports’ for accepting this article for publication. This is a rigorously peer reviewed journal which is on all major global scientific data bases. I note the review process was prompt, thorough and professionally critical. It gave us an insight into a number of important scientific/statistical issues. The review prompted us to review the relevant literature again and look at the limitations of the study. The peer reviewers were open, clear in the instructions and the editorial team was very prompt in their communication.
This journal certainly publishes quality research articles.
I would recommend the journal for any future publications.
Dr Farooq Wandroo
Dear Jessica Magne, with gratitude for the joint work. Fast process of receiving and processing the submitted scientific materials in “Clinical Cardiology and Cardiovascular Interventions”. High level of competence of the editors with clear and correct recommendations and ideas for enriching the article.
Dr Anyuta Ivanova
We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
Dr David Vinyes
My article, titled 'No Way Out of the Smartphone Epidemic Without Considering the Insights of Brain Research,' has been republished in the International Journal of Clinical Case Reports and Reviews. The review process was seamless and professional, with the editors being both friendly and supportive. I am deeply grateful for their efforts.
Gertraud Teuchert-Noodt
To Dear Erin Aust – Editorial Coordinator of Journal of General Medicine and Clinical Practice!
I declare that I am absolutely satisfied with your work carried out with great competence
in following the manuscript during the various stages from its receipt,
during the revision process to the final acceptance for publication.
Thank
Prof. Elvira Farina
Dr Elvira Farina
Dear Jessica, and the super professional team of the ‘Clinical Cardiology and Cardiovascular Interventions’
I am sincerely grateful to the coordinated work of the journal team for the no problem with the submission of my manuscript: “Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report).”
The review process by 5 experts was fast, and the comments were professional, which made it more specific and academic, and the process of publication and presentation of the article was excellent.
I recommend that my colleagues publish articles in this journal, and I am interested in further scientific cooperation.
Sincerely and best wishes,
Dr. Oleg Golyanovskiy.
Dr Oleg Golyanovski
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.