AUCTORES
Globalize your Research

case report | DOI: https://doi.org/10.31579/2690-4861/769
Professior, Oral and Maxillofacial Surgery, Dept of Dental Surgery & OHS, AFMC, Pune, Maharashtra.
*Corresponding Author: Yadav Rekha Chintamani, Graded Specialist, Oral & Maxillofacial Surgery, CMDC, Udhampur, J&K.
Citation: Kapil Tomar, Yadav Rekha Chintamani, Indranil Deb Roy, (2025), Rhinoplasty: Enhancing Facial Harmony and Nasal Proportions, International Journal of Clinical Case Reports and Reviews, 25(3); DOI:10.31579/2690-4861/769
Copyright: © 2025, Kapil Tomar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 March 2025 | Accepted: 08 April 2025 | Published: 15 April 2025
Keywords: rhinoplasty; costochondral graft; trans-columnellar
Considered to be one of the most technically challenging procedures, rhinoplasty as a surgery has not only a functional component, but it also encompasses aesthetic aspects. Operating in one of most easily perceptible areas of the human body, the face, effects of rhinoplasty are plainly visible to the general population and a nearly impossible arena that can be disguised or placed out of public view. This case series presents two cases of open rhinoplasty: A 23yrs old male who desired aesthetic correction of nasal deformity & a 30yrs old female with post-traumatic residual nasal deformity due to sustained maxillofacial injuries in an alleged incidence of RTA. A detailed history and thorough clinical examination in various profile views, diagnosis of nasal deformity necessitating rhinoplasty was made. Both the cases were undertaken for open rhinoplasty using costochondral graft under GA after routine hematological workup. There was post-operative restoration of desired nasal contour.
Over the last decade, rhinoplasties have increased by leaps and bounds to fulfill functional and cosmetic demands.
The etiologies causing a deficient or deformed nasal dorsum can be either congenital, iatrogenic or traumatic [1]. Achieving a symmetric, smooth, stable, and desired nasal dorsum that fulfills the criteria of adequate form, function, and patient expectation remains a principle challenge during primary or secondary rhinoplasties. Addressing the key areas of nasal complex like internal nasal valve, nasal septum and inferior turbinates have paved a way for getting the best functional out comes of various rhinoplasty surgical modalities [2].
While the negative results can have an enormous adverse psychological after-effect & lasting impact on the patient, surprisingly, the positive results my easily be forgotten.
The search for precise understanding of the nasal anatomy and its importance in facial esthetics can be dated back to more than 500 years ago, when Leonardo da Vinci illustrated the importance of facial proportions and beauty [3-6]. Although various alloplastic materials provided a good alternative, they were also associated with complications of thinning of skin over implants, infection, translucency of implants & chronic pain. Autologous grafts, on the other hand, such as costal bone and cartilage have been used effectively with varying effects and relatively fewer complications [2,7]. It is reported that with proper carving and meticulous construction, augmentation rhinoplasty using costo-chondral material can produce excellent results [1,7,8].
We have highlighted two such cases of dorsal nasal augmentation through use of costochondral graft.
A 23 years old male, dissatisfied with appearance of his nose, reported to us seeking professional consultation and required necessary intervention. Clinical examination revealed flattened bridge of nose with convex dorsum, flattened tip lobule, loss in convexity of alar lobule and decreased tip projection, all giving the impression of parrot beak appearance (Figure 1).
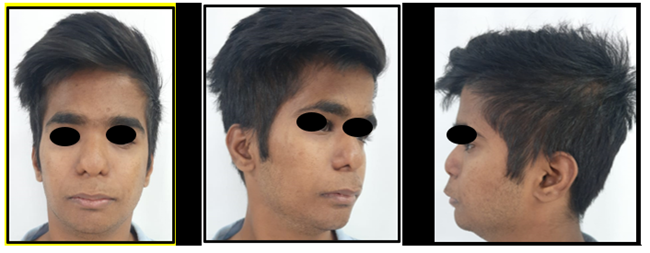

Figure 1: Pre-Operative appearance of depressed nasal dorsum (Case 01)
Case 2: A 30yrs old female patient, an operated case of pan-facial trauma at the same center, presented with post-traumatic secondary residual nasal deformity. Problem list included depressed nasal bridge, loss of nasal projection and deviation of nose towards left side (Figure 2).

Figure 2: Pre-Operative appearance of depressed nasal dorsum (Case 02)
After detailed history and thorough clinical examination focusing on comprehensive nasal analysis, informed written consent was taken from patient for open structure rhinoplasty approach.
Costochondral graft harvesting was done following the standard procedure (Fig 3). The 5th rib was chosen in both the cases. Skin incision was placed on the region over the right rib for about 3 cm in length. After incising through the proposed incision line over skin, blunt dissection was performed to carefully divide the overlying breast tissue. Any bleeders, so encountered, were cauterized with cautery. Dissection proceeded through fascia, separating muscle fibers hemostat. The remaining soft tissue was cleared off the rib for visualization. The perichondrium was
incised along the periphery of the rib and an elevator was used to remove this 5-to 10-mm strip of perichondrium. Cartilaginous part of the rib was dissected away from the perichondrium circumferentially while exercising caution to avoid injuring the perichondrium. An incision, halfway through the rib just medial to the osteo-chondral junction, was made based on the required length of cartilage. The segment of costal cartilage was removed and set aside. After checking for any injury, closure was performed in layers. The costochondral graft was carved sequentially over long time period so as to allow the natural warping tendencies of each piece to be demonstrated. The dorsal is best carved from the central core of the rib in a centric fashion [7].
The nasal region was intra-nasally approached via the trans-columnellar incision [Figure 4]. Beginning with an inverted V shaped incision between the upper and lower cartilage, dissection was carried up onto the middle nasal vault, staying in a plane immediately adjacent to the cartilage. A periosteal elevator was used to create a small sub-periosteal pocket over the bony dorsum in the midline. The superior aspect of this pocket should lie at about the midpupillary line and correspond to the proposed nasal starting point. This place was created with a notch (inverted C) so that the costochondral graft sits over this notch. Nasal dorsal height is based on the tip projection. The costochondral graft is often a canoe-shaped graft. Depending on the degree of augmentation required, the thickness of graft could be increased by staking making sure of beveling edges. The graft was then placed into the narrow dorsal pocket created and stabilized by suturing with 4-0 PDS (polydioxanone) to the L-strut framework for splinting the deviated caudal septum.
Before suturing, careful inspection and palpation of graft is performed to ensure the graft is in midline, symmetric, and without irregularities (Fig 5) [7]. There was warping encountered in one of the cases in immediate post-operative period, leading to graft exposure. Re-intervention was immediately advised considering patient’s apprehension and expectation and correction was done. Post-operative follow-ups were done to assess surgical outcomes (Figure 6).

Figure 3: Costochondral graft harvesting
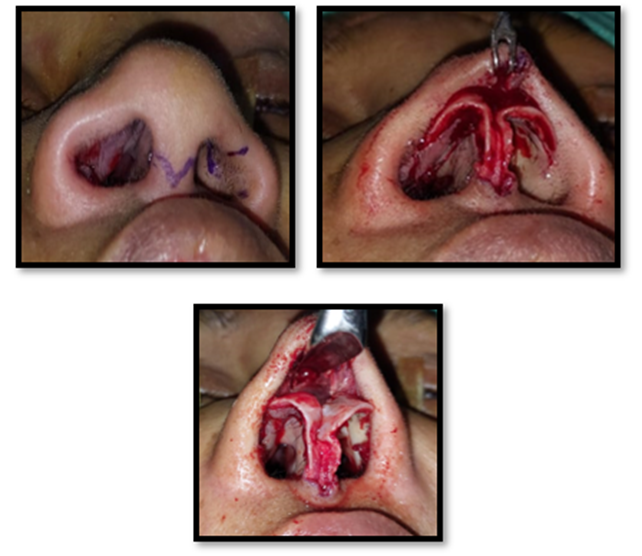
Figure 4: Open Rhinoplasty via Trans-columnellar incision

Figure 5: Verification of graft position intra-operatively and closure
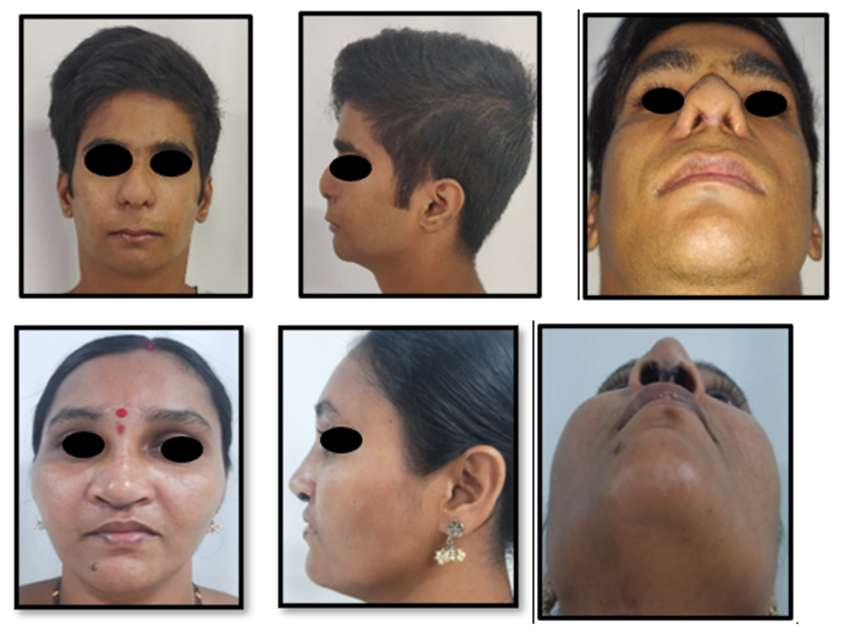
Figure 6: Post-Operative results
Requiring a sound understanding of the nasal anatomy and surgical maneuvers, rhinoplasty still remains one of the most challenging surgical procedure to master till date. Undoubtedly, no area of the human body other than face is more important. Since even slightest of the discrepancies in mere millimeters can have a significant positive & negative impact in these surgical procedures, it is imperative for Esthetic as well as Oral & Maxillofacial Surgeons to understand ideal facial proportions & have a thorough understanding of the nasal anatomy that will eventually dictate an aesthetically & functionally pleasing surgical outcome [9].
It was Leonardo da Vinci who established esthetic standards that in use till date [9]. He divided the face into horizontal thirds by parallel lines drawn at the hairline, the eyebrows, the nasolabial angle and, finally, the mentum. He emphasized that a good nose should not be longer than the middle third. Likewise, he divided the face into fifths by drawing vertical lines that defined spaces as wide as one eye; he pointed out that the nose should not be wider than the middle space so defined (Figure 7) [9].
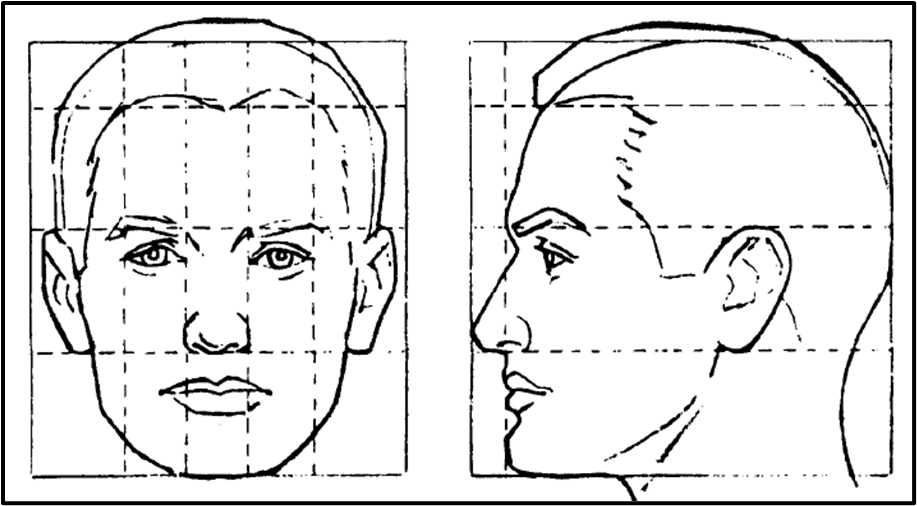
Figure 7: Da Vinci’s ideal proportions
Over the centuries ever since then, anatomists have attempted in studying and describing the relative spatial relationships of the nasal architecture. Usually when one anatomic part is described relative to another, the standard anatomic descriptors are used, including anterior, posterior, superior, and inferior. Specifically, when referring to nasal relationships, additional terms are used including dorsal, basal, caudal, and cephalic (Figure 8) [3,10,11,12].

Figure 8: Relative spatial relationships
This complex and fascinating structure of the human face continually provides challenges to surgeons, but the impact of a successful procedure will have lifelong benefits to the receiving patient.
The debate between the choice of grafting materials, i.e. between alloplasts and auto grafts, has nearly always favored auto grafts in the form of costochondral graft. From mild to severe defects demanding reconstruction, costochondral graft provides strong grafts to augment or support the nasal dorsum, tip, or septum. Possible disadvantages include donor site morbidity, increased operative time, and a risk of graft warping [1].
In their series of 46 cases, Gibson & Davis used concentric segments of costochondral graft to minimize warping [13]. It is well documented that the change in shape of the costochondral graft with time can be attributed to its dynamic composition of protein-polysaccharides with cartilage that produces internal tensile stresses [14]. Also, central portions of costochondral graft warp less than peripheral portions [15,16]. It has been proved that warping of costochondral graft can be effectively reduced by systematic, concentric carving of cartilage from the center of rib segments. The inherent forces of warping appear to act more in the dorsal-ventral dimension of costochondral graft, but not clinically manifesting owing to compensation by thick skin. But the side-to-side warping is more clinically evident due to less soft tissue resistance in this dimension. Similarly, the end time of warping of costochondral graft is still debated [15].
While the esthetic rhinoplasty procedures can fit in various surgical techniques, addressing post-traumatic nasal deformity can be more challenging. Nasal bone fractures are the most common fractures of the facial skeleton. Frequently patients are treated without inadequate preoperative assessment, being closed manipulation an insufficient procedure for definitive treatment. Problems of the traumatic nose include complex osseocartilaginous defects, alteration of soft tissue planes and the loss of potentially donor areas for cartilage. Many patients who suffer mid-face trauma, concomitantly also suffer from nasal deformity/deviation and nasal airflow impedance. There are three specific regions within the nose which may impede airflow: nasal septum, internal nasal valves, and inferior turbinates. When indicated, by appropriately addressing the before mentioned key regions of the nasal complex, the majority of patients (90.5%) will have no subjective complaints of difficulty breathing from their nose, following a post-traumatic rhinoplasty [17].
Of the various surgical techniques elaborated in literature, open rhinoplasty allows directs vision and complete exposure of the surgical field, offering an added advantage in fractures sequelae of pot-traumatic cases. Its advantages include a wide surgical exposure, without distortion of the nasal tip, a direct and easier handling of the alar cartilages, and an opportunity for accurate modelling and fixation of grafts. It is also especially helpful as a teaching procedure for trainees. Its disadvantages, though minor should be considered and include external scarring, long-term swelling of the tip and numbness in the columella [18].
A graceful nasal contour can be accomplished in aesthetic surgery by preserving and assessing the anatomical nasal lines and also keeping the functional aspect in mind. In cases of disfigured victims following RTA, nasal reconstruction or rehabilitation procedures becomes really challenging. Of the various methods & techniques available, structural rhinoplasty with costal cartilage grafts permits a good quantity of cartilage in the manufacture of allowing a safe nasal reconstruction of the deformed nasal dorsum.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.





























































