
Case Report | DOI: https://doi.org/10.31579/2642-1674/007
*Corresponding Author: lokesh rana, Department of Radiodiagnosis DRPGMC, Tanda, Kangra, H.P., India
Citation: lokesh rana, Portal Annular Pancreas with portal cavernoma formation with associated dorsal pancreatic agenesis-A rare case report, J Clinical Imaging and Interventional Radiology, 2(1) Doi: 10.31579/2642-1674/007
Copyright: © 2018 lokesh rana. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 July 2019 | Accepted: 18 July 2019 | Published: 17 July 2019
Keywords: Keywords
Portal annular pancreas is a uncommon congenital anomaly resulting from fusion of the pancreatic parenchyma around the portal vein. Its causing portal cavernoma formation and association with dorsal pancreatic agenesis is rare
Case report We report a 51-year-old female who underwent contrast enhanced computed tomography for vague right hypochndrial pain.On CECT abdomen images there was presence of rind of pancreatic tissue around the portal vein causin its luminal narrowing with proximal dilation of portal vein tributaries with cavernoma formation.There was also presence of agenesis of dorsal pancreas in this patient.Conclusion This variant of portal annular pancreas with cavernoma formation associated with dorsal pancreatic agenesis has not yet been reported and we propose a new CT classification of the same.
Portal annular pancreas (PAP) is an uncommon and under-recognized congenital anomaly of the pancreas and with cavernoma formation with associated dorsal pancreatic agenesis is rarest and not been reported in the literature. In contrast to a conventional annular pancreas in which the pancreatic tissue encircles the second part of the duodenum, portal annular pancreas is characterized by encasement of the portal vein by rind of pancreatic parenchymal tissue1,2.
We noted, on an axial abdominal computed tomography study of a 69-year-old female with chronic vague pain in right hypochondriac region, anomalous pancreatic parenchyma encircling the main portal vein with proximal dilation of the portal vein tributaries with consequent cavernoma formation. There was also presence of agenesis of dorsal pancreatic tissue3,4,5,6.(Fig.)
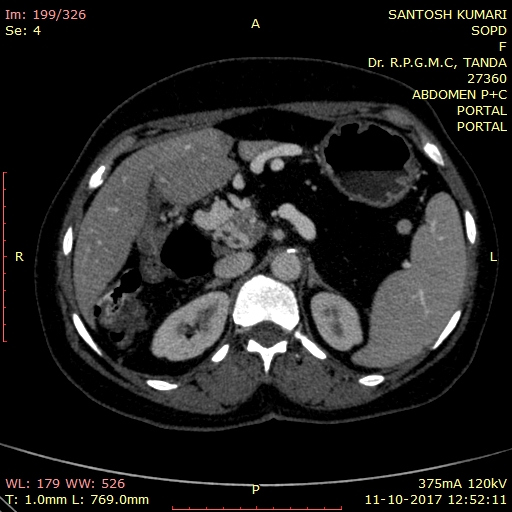
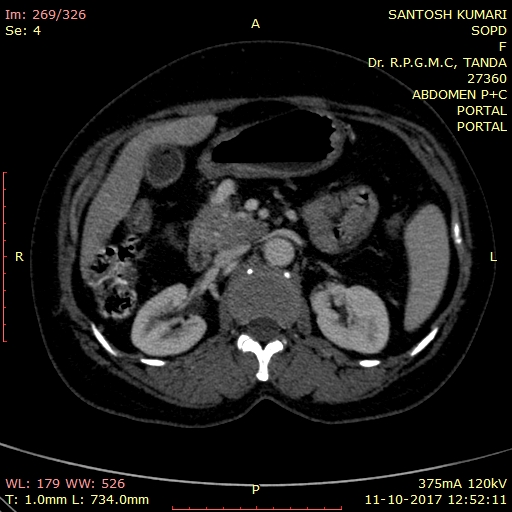
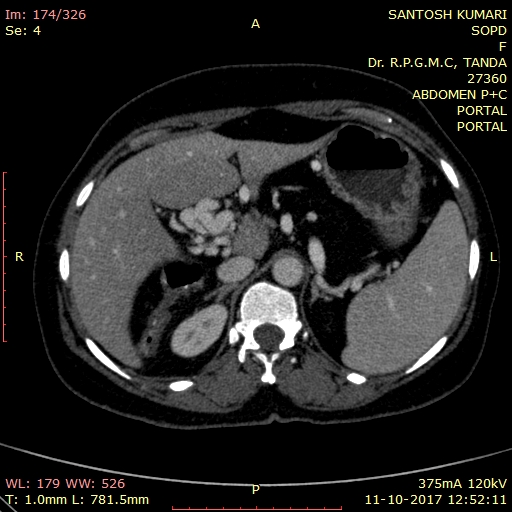
CECT images portal venous phase of 31 year old female showing(fig a) a rind of pancreatic tissue around portal vein(arrow) causing its luminal narrowing. There is presence of dorsal agenesis of pancreas(fig b) with dependant viscera sign(arrow).This is Type IV portal annular pancreas according to the new classification described in the text.Fig c shows dilated proximal portal channels with cavernoma formation(arrow).
Pancreas develops from a ventral and a dorsal bud of the duodenum2,8,9. The ventral bud forms the major part of the head and the uncinate process, whereas the dorsal bud forms upper part of the head, the body, and tail of the pancreas. The ventral bud rotates posteriorly during the 7th week of gestation to fuse with the dorsal bud so as to form the fully mature gland10. Rarely, this fusion occurs to the left of the mesenteric or portal vein, resulting in a encircling pancreatic parenchymal tissue around the portal vein. This has been referred to as the portal annular pancreas. Karasaki et al1. and Ishigami et al 13 in their studies concluded that the prevalence of portal annular pancreas is not extremely low but is not readily recognized on preoperative imaging due to lack of adequate knowledge and awareness of this uncommon variant but its association with dorsal pancreatic tissue has not been reported yet11,12,13.
Imaging plays a pivotal role in the diagnosis of portal annular pancreas and contrast-enhanced multi-detector computed tomography (MDCT) is considered sufficient enough to establish the diagnosis. Joseph et al14. have classified PAP into 3 types. In type I the ventral bud of the pancreas fuses with the dorsal bud posterior to the portal vein with a retroportal pancreatic duct (as is seen in the present case); type II has concomitant pancreas divisum; and type III is when the uncinate process alone is involved and the pancreatic duct is seen anterior to the portal vein (anteportal pancreatic duct)3,7,14,16.
Another classification describes this entity as suprasplenic (commonest), infrasplenic, and mixed type based on the fusion of uncinate process with the body posteriorly above or below the level of the splenoportal confluence. It may be associated with the abnormal course of pancreatic duct (retroportal pancreatic duct) or pancreatic divisum17,18.
We propose a new classification of this entity with two groups.1,3,19,20
Group A-Portal annular pancreas(PAP) without complications
Group B-Portal annular pancreas(PAP) with complication of potal hypertension,pancreatitis,obstructive biliopathy etc.
Type I-Ventral bud fuses with the dorsal bud posterior to portal vein forming a rind of pancreatic tissue around portal vein
Type II-Pancreatic divusum
Type III-Anteportal pancreatic Duct
Type IV-Associated dorsal pancreatic agenesis
Our case is type IV and computed tomography scan is usually adequate for diagnosing this anomaly, which can be demonstrated by continuity of the extension of the uncinate process into the body of the pancreas in more than 2 slice however, the presence of the anomaly of pancreatic ducts can also be suggested by demonstrating the abnormal course of the pancreatic duct when present which can be depicted on MRCP or ERCP21,22.
PAP is a rare anomaly and cavernoma formation with associated dorsal pancreatic agenesis more rarer. We emphasize on the new classification system which lay stress on complication associated with it and co-existant congenital anomalies of pancreas.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
