AUCTORES
Globalize your Research

Review Article | DOI: https://doi.org/10.31579/2692-9406/184
North Manchester General Hospital, Department of Urology, Delaunays Road, Crumpsall, M8 5RB, Manchester, United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Department of Urology, Delaunays Road, Crumpsall, M8 5RB, Manchester, United Kingdom.
Citation: Grey Venyo AK, (2024), Ossification in Human Penis: Review and Update, J. Biomedical Research and Clinical Reviews. 9(2); DOI:10.31579/2692-9406/184
Copyright: © 2024, Anthony Kodzo-Grey Venyo. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 March 2024 | Accepted: 22 March 2024 | Published: 29 March 2024
Keywords: ossification in penis; bone in penis; congenital; peyronies disease; curvature of penis; diabetes mellitus; trauma; gout; pathology; excision
Human penile ossification is a rare urological condition with about 40 cases reported in the literature. While bone is essential for penetrative intercourse in many non-human mammals, human penile ossification appears to be part of a metaplastic process occurring after injury or trauma. Conditions such as Peyronie’s disease, diabetes mellitus, local trauma, and end-stage renal disease have been associated with this entity Human penile ossification may be asymptomatic or may be associated with previous trauma to the penis, or could on rare occasions be congenital. Ossification of the penis may be asymptomatic or may present with a lump in the penis, pain in the penis, or pain and curvature of penis in association with erection. Radiology imaging does demonstrate the ossification within the penis and complete excision of the ossification area of the penis tends to be associated with resolution of the symptoms. In the rare situation of osteosarcoma of the penis, surgical excision of the entire lesion does constitute an appropriate treatment.
Belshoff et al. [1] stated the ensuing:
Considering the rarity of penile ossification, it would be envisaged that majority of clinicians globally and well as most patients globally would not be familiar with the fact that bone or ossification could on rare occasions be found within the penis and they would tend not to be familiar with the manifestation, diagnosis, management and outcome of penile ossification. The ensuing article on penile ossification or bone tissue within the penis is divided into two parts: (A) Overview which has discussed general overview aspects of penile ossification, and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to penile ossification.
Aim
To review and update the literature on bone or ossification within the human penis.
Methods
Internet data bases were searched including Google; Google Scholar; Yahoo; and PUBMED. The search words that were used included: Bone in penis; penile ossification; OS Penis; and Penile OS. Fifty-seven (57) references were identified which were used to write the article which has been divided into two parts:
[A] OVERVIEW
Definition and General Statements [11]
Terminology
Aetiology
The ensuing summations had been made regarding the aetiology of bone in the penis: [11]
Presentation
Clinical Assessment Findings
Miscellaneous Laboratory Investigations
Urine
Blood tests
Haematology blood tests
Biochemistry blood tests
Plain X-ray
Ultrasound Scan
Computed Tomography (CT) scan
Magnetic Resonance Imaging (MRI) scan
Treatment
Pathology Examinations
Differential Diagnosis
Outcome
[B] Miscellaneous Narrations And Discussions From Some Case Reports, Case Series, And Studies Related To Bone Within The Penis
Belshoff et al [1] reported a 65-year-old man who was referred to their urology department for an eight-year history of dorsal curvature of his penis with erections. He had described a near 90-degree curvature, which had been stable for several years and was refractory to in-office verapamil injections. He did not have any difficulty obtaining erections; nevertheless, they were painful and bothersome. He found sexual intercourse to be also difficult and painful for both him and his partner due to the curvature. His medical and surgical history was otherwise unremarkable. Upon his examination, his penis was uncircumcised with a palpable, firm plaque along the dorsal aspect of his midshaft of penis measuring about 2.5 cm by 1.5 cm. A penile Doppler ultrasound was undertaken, which demonstrated a broad, linear, sheet-like densification of the dorsal tunica albuginea extending from the base of the penis along most of the shaft, predominantly along the right side (see figure 1).
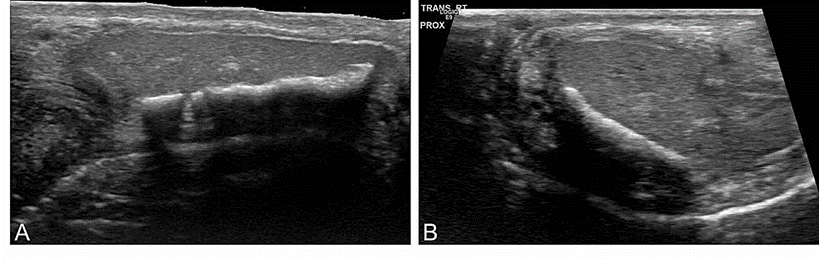
Figure 1: Penile Doppler ultrasound imaging demonstrating a 2.5-cm dorsal density with acoustic shadowing
A) Longitudinal view of the right corpora. B) Transverse view primarily of the right corpora Reproduced from [1] under the Creative Commons Attribution License In view of the extensive degree of plaque and the impact upon his quality of life, he was taken to the operating theatre for partial excision and grafting. Intraoperatively, the large, firm ossified plaque was immediately visualised, and care was taken to excise this while preserving the neurovascular bundles. The corporal defect was closed utilising a bovine pericardial graft (Coloplast, Minneapolis, MN). Upon intraoperative induction of an artificial erection, the partial curvature was still apparent, which necessitated placement of two tunica albuginea plication sutures along the ventral shaft. The penile curvature was corrected to 10 degrees dorsally at the end of the procedure. The remainder of his hospital course was unremarkable, and he was discharged home the same day.
His postoperative course was documented to be also uneventful, with minimal residual curvature noted during his two-month follow-up assessment. He denied any erectile dysfunction and was then able to obtain satisfactory erections without medications. He was sexually active with his partner and he denied pain or difficulty with intercourse.
Macroscopy pathology examination of the excised tissue had demonstrated multiple tan-white, elongated segments of glistening tissue with central areas of calcification that measured in aggregate 3.2 cm by 1.6 cm by 1.1 cm. The tissue was examined after decalcification. The hematoxylin and eosin histology sections revealed a centrally located bony tissue encompassed by penile fibrous tissue (see figure 2A). The bony tissue exhibited features of lamellar bone under polarized light (see figure 2B). No inflammation was found present within the lamellar bone and adjacent fibrous tissue.

Figure 2: Microscopic examination
A) H&E section showing bone surrounded by unremarkable stroma. B) The same section examined under polarized light showing lamellar bone. Original magnification: 300x H&E: hematoxylin and eosin. Reproduced from [1] under the Creative Commons Attribution License.
Belshoff et al. ]1] made the ensuing educative discussions
Belshoff et al. [1] made the ensuing conclusions:
In 2007, de Arruda et al. [17] stated the ensuing:
de Arruda et al. [17] reported a 59-year-old white man who had manifested with a one-year history of slight pain upon erection and during intercourse. He also did complain of hard plaque near the base of his penis. One year preceding his manifestation, he had sustained blunt trauma during intercourse. Examination of his penis demonstrated a fixed firm mass which had extended over the proximal third of his penile shaft, that measured 3.0 x 3.0 x 2.0 cm and which had involved his corporal sponge, without surface extension. He did not have any impotence or other relevant clinical finding. Radiography on the penis had demonstrated irregular calcification in the same position as the palpable mass and in the septum of the proximal inner third of his penis. de Arruda et al. [17] stated that:
Frank et al. [18] stated the following:
Frank et al. [18] reported an additional case of ossification of the penis in 1989.
Yilmaz et al. [6] stated the following:
Yilmaz et al. [6] reported a 54-year-old man, who had presented to the urology office with a 1-year history of a painless hard proximal penile masses which had involved one-third of the length of his corporal bodies bilaterally. He was neither sexually active nor bothered by symptoms from this penile lesion; he manifested; nevertheless, for workup concerning the possibility of malignancy. He denied having any history of trauma or family history of genitourinary malignancy. He also denied having penile pain, dysuria, irritative voiding symptoms or any other subjective complaints. To the patient’s knowledge, the hard mass had been present for many years and had gradually increased in size over time. His clinical examination demonstrated a mobile, rock-hard, calcified mass that was palpable within the base of his penis circumferentially which had involved both proximal corpora. The result of his digital rectal examination was normal and no inguinal nodes were palpable on examination. The results from his routine laboratory assessments were normal. He had a magnetic resonance imaging scan of his pelvis with gadolinium which failed to demonstrate any corporal abnormalities, and no pelvic lymphadenopathy was seen upon the imaging. At that point, the decision was taken to undertake a cystoscopy and excisional biopsy of the calcified mass at the base of his penis. His cystoscopy demonstrated a normal urethra, urinary bladder mucosa, and prostate, which had confirmed that the plaque was external to the urethra. After degloving the phallus, the hard calcified proximal corpora were easily palpated and felt to be entirely replaced by a calcific process. An excisional biopsy was undertaken of the right corpora, with minimal bleeding noted from the calcified corporal body. Histopathology examination of this specimen demonstrated metaplastic ossification to lamellar bone with eosinophilic ossified matrix, lacunar spaces and haversian vascular canals characteristic of bone (see figure 3).

Figure 3 A: Photomicrograph of histological section from the lesion, showing metaplasia of bone tissue in the corpus cavernosum. B: Osteoblastic rimming around bone tissue C: Osteoblasts. D: Multinucleated osteoclasts.
Reproduced from [6] under the Creative Commons Attribution License.
Yilmaz et al. [6] made the ensuing educative discussions:
Yilmaz et al. [6] made the following conclusions:
Villani et al. [13] stated the following:
Homero Oliveira de Arruda et al. [24] reported a 59-year-old white man, who was referred with a one-year history of slight pain upon erection and during sexual intercourse. He also had complained of hard plaque near the base of his penis. One year earlier, he had sustained blunt trauma during sexual intercourse, after which he began to experience pain when the penis became turgid. He did not have any history of metabolic disorder or erectile impotency. Examination of his penis demonstrated the presence of a firm fixed mass, which had extended over the proximal third of the shaft of his penis. It was irregular, mass that measured 3.0 cm x 3.0 cm x 2.0 cm, and which had involved the corporal sponge without surface extension. There were no other relevant clinical findings. The results from his routine laboratory evaluations were normal. Radiography on his penis demonstrated irregular calcification within the same position as the palpable mass and in the septum of the proximal inner third of the penis (see figures 4 and 5). The calcified mass was excised surgically via a dorsal midline incision of the tunica albuginea, which had extended across the corpus cavernosum on both sides. The defect of the corporotomy was closed utilising a watertight running 4-0 vicryl suture, without grafting. A quick examination of the specimen demonstrated an irregular mass of greyish brown tissue with hard white calcified foci. His postoperative course was uneventful and the patient reported a full straight erection without pain. Histopathology examination of the specimen demonstrated cancellous bone encompassed by dense collagen tissue. Homero Oliveira de Arruda et al. [24] made the ensuing educative discussions:
Homero Oliveira de Arruda [24] concluded that:
Their understanding of this case was that the ossification in their patient probably had developed as a consequence of unusual repair of the tunica albuginea, following some blunt trauma sustained during sexual intercourse.
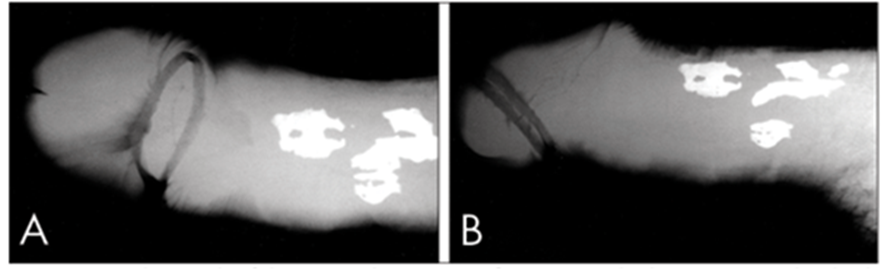
Figure 4. Radiograph of the penis showing ossification inside the septum and in both corpora cavernosa. A: Frontal view; B: Sagittal View. Reproduced from [24] under the Creative Commons Attribution License.

Figure 5. Photomicrograph of histological section from the lesion, showing metaplasia of bone tissue in the corpus spongiosum. Reproduced from [24] under the Creative Commons Attribution License.
Ustriyana et al. [28] stated the following:
Ustriyana et al. [28] reported that human MPPs (n = 11) were surgically excised, and the organic and inorganic constituents were spatially mapped utilising multiple high-resolution imaging techniques. Multiscale image analyses resulted in spatial colocalization of elements within a highly porous material with heterogenous composition, lamellae, and osteocytic lacuna-like features with a morphological resemblance to bone. The lower (520 ± 179 mg/cc) and higher (1024 ± 155 mg/cc) mineral density regions were associated with higher (11%) and lower (7%) porosities in MPP. Energy dispersive X-ray and micro-X-ray fluorescent spectroscopic maps in the higher mineral density regions of MPP had revealed higher counts of calcium (Ca) and phosphorus (P), and a Ca/P ratio of 1.48 ± 0.06 similar to bone. More importantly, higher counts of zinc (Zn) were localized at the interface between softer (more organic to inorganic ratio) and harder (less organic to inorganic ratio) tissue regions of MPP and adjacent softer matrix, indicating the involvement of Zn-related proteins and/or pathways in the formation of MPP. In particular, dentin matrix protein-1 (DMP-1) was colocalized in a matrix rich in proteoglycans and collagen that contained osteocytic lacuna-like features. Ustriyana et al. [28] made the ensuing conclusion and statement of significance:
Hsu et al. [14] stated that in order to elucidate the anatomic distal ligament of the human glans penis and associated clinical implications, they compared the structures of the glans penis and corpora cavernosa in dogs, rats, and humans. From May 2001 to March 2003, gross dissection, microscopic examinations, and stains for elastic fibres and collagen subtypes were made in the penises of 11 adult human male cadavers, 7 dogs, and 5 rats. A distal ligament in the human glans penis replaced the os penis which is present in dogs or rats, also termed the baculum, but retained collagen types I and III as common structural and interlocking components, respectively. The intercavernosal septum was complete, and intracavernosal pillars (ICPs) were abundant in dogs, absent in rats, and moderately developed in humans. A tunica with numerous elastic fibres existed to fulfil the requirements of erectile function in humans but not in dogs or rats, since it was essential for establishing tissue strength to serve as a buttress. They would conclude as follows:
Athanazio et al. [12] reported a 19-year-old patient, who had noticed a deep nodule within the dorsal side of his penis 2 years preceding his presentation. The nodule had been assessed clinically in other service. During this period, no skin lesions were noted. Over the preceding last months, the lesion had rapidly grown causing ulceration in his dorsal skin and invaded corpora cavernosa and corpus spongiosum (as evaluated by imaging studies). An incisional biopsy was undertaken showing a high-grade neoplasm with many non-neoplastic osteoclast-type multinucleated giant cells. An immunohistochemical panel study including SATB2 positivity in mononuclear cells had favoured sarcoma over sarcomatoid carcinoma. A partial penectomy without lymphadenectomy was undertaken (see figure 6) demonstrating a large tumour with pushing borders and 5-cm maximum diameter.

Figure 6: Gross appearance of penile osteosarcoma. Clinical appearance before surgery (A) and after resection and formalin fixation (B). Cut surface of the specimen. Fleshy tumour involving corpora cavernosa and corpus spongiosum. Upper left section shows uninvolved margin and bottom right shows the uninvolved distal glans (C). Reproduced from: [12] under the Creative Commons Attribution License.
The microscopy pathology examination findings of the penectomy specimen mirrored those of the incisional biopsy. The entire tumour was submitted for microscopic evaluation. The tumour had demonstrated highly pleomorphic sarcoma with epithelioid and fusiform cells intermixed with numerous non neoplastic osteoclast-type multinucleated giant cells (see figure 7). Necrosis was identified within < 10% of the whole tumour volume. There was brisk mitotic activity with 30 mitoses per 2 mm2. Angiolymphatic invasion was also identified. There was no clearcut foci of osteoid matrix; nevertheless, some foci of tumour cells demonstrated lace-like or trabecular deposition of matrix which was difficult to discern from collagenous stroma (see figure 8).

Figure 7: High-grade sarcoma with numerous non neoplastic osteoclast-type multinucleated giant cells (A: HE, 10x). It shows brisk mitotic activity (B: HE, 100x) and frequent atypical mitoses (C: HE, 400x). The whole tumour was submitted for histological analysis and few areas of equivocal osteoid matrix production were observed (C: 400x, HE stain). Atypical mononuclear cells show diffuse nuclear staining for SATB2 (E: 100x and F:400x) while only osteoclast-type multinucleated giant cells stained for marker of histiocytic differentiation, CD68 (G: 400x) Reproduced from [12] under the Creative Commons Attribution License

Figure 8: Equivocal areas of osteoid formation that may yield differential diagnosis with collagenous stroma (HE – A, 400x; B, 400x, C, 40x; D, 400x). Reproduced from [12] under the Creative Commons Attribution License
In both biopsy and penectomy specimen, atypical mononuclear cells were found to be diffusely positive for SATB2 (a marker of osteoblastic differentiation), CD99 and vimentin. These cells were negative for pan-keratin, GATA3, EMA, SOX10, S100 and ERG. Desmin was focally expressed. CD68 was expressed only in multinucleated giant (osteoclast-like) cells. The tumour cells had exhibited preserved INI1/SMARCB1 expression. See immunohistochemical photomicrographs in Figure 9.

Figure 9: Immunophenotype of a giant-cell rich penile osteosarcoma: no pan-keratin [removed]A, 40x), CD99 expression restricted to neoplastic cells (B, 40x), SATB2 expression in tumour cells (C, 40x; D, 400x), and CD68 positivity in giant osteoclast-type cells (E, 40x) Reproduced from [12] under the Creative Commons Attribution License
The radiology imaging studies had excluded any bone primary tumour. The patient had developed lung metastases after ten months of his follow up.
Athanazio et al. [12] made the ensuing educative discussions:
Athanazio et al. [12] made the ensuing conclusions:
Wu et al. [33] stated the following:
Wu et al. [33] reported a 68-year-old man, who had manifested with a tender subcutaneous nodule of his penis. The nodule had localized pain and grown from about 0.3 cm × 0.3 cm × 0.3 cm to 1.2 cm × 0.8 cm × 0.5 cm in a year. Upon clinical examination, a 1.2 cm × 0.8 cm × 0.5 cm mass was palpated that measured 0.8 cm to the right to coronary sulcus. There was no red swelling of the skin and abnormal temperature. The edge of the mass was clear. The mobility of the mass was poor. The scrotum and testis of the patient were normal, and there was no touched intumescent lymph node in his inguinal region. The operation was undertaken in May, 2009. Wu et al. [33] stated that the patient received 1% Lidocaine injection at the root of his penis and the surgery was undertaken. The skin and subcutaneous tissue were dissected to segregate the mass. The tumour was noted to have slightly adhered to the encompassing tissue but did not invade to tunica albuginea. Finally, the mass was excised and a histological diagnosis was made. The patient was followed up for 10 months, and then lost to follow-up. Macroscopy examination of the specimen demonstrated that the neoplasm without envelope was greyish-white, greyish-pink and 1.5 cm×1 cm × 1 cm. The cut surface of the mass was greyish-white and rigid, and had sense of grit and no weaving shapes.
Microscopy examination of the specimen demonstrated that the cells within the tumour were widespread and irregular, mainly spindle and ovoid. The cytoplasm of the cells is basophilic. The nuclei were obviously atypical, mostly clostridial form and polygons. Massive bone matrix which coexisted with multinucleated giant cells could be found everywhere within the tumour. The tumour cells were noted to be in palisade arrangement and most commonly seen in and around the bone matrix. In some instances, 3.5 to dozen nuclei could be visualised in a single multinucleated giant cell.
Wu et al. [33] made the ensuing discussions:
Conflict of Interest – None
Acknowledgements
Acknowledgements to:
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
