
Research Article | DOI: https://doi.org/10.31579/2692-9422/011
1Consultant neonatology, Al Jalila Children's Specialty Hospital, Dubai health, UAE.
2Specialist neonatology, Latifa Hospital, Dubai health, UAE.
3Rehabilitation, Physiotherapy1, Al Jalila Children's Specialty Hospital, Dubai health, UAE.
4Consultant pediatric, Al Jalila Children's Specialty Hospital, Dubai health, UAE.
*Corresponding Author: Munira Mahmoud Almaazmi, Consultant neonatology, Al Jalila Children's Specialty Hospital, Dubai health, UAE.
Citation: Munira M. Almaazmi, Ahmed Elgendy, Rocky R. Sonale, Mohamed Elmesserey. (2026), Non-Surgical Scoliosis Management in Pediatric complex cases: A Pathway to Improved Respiratory Function, Neurodegeneration and Neurorehabilitation, 5(1): DOI:10.31579/2692-9422/011
Copyright: © 2026, Munira Mahmoud Almaazmi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 April 2026 | Accepted: 17 April 2026 | Published: 21 April 2026
Keywords: conservative treatment; pediatric scoliosis; pulmonary outcomes; respiratory function
Background: Pediatric scoliosis can alter thoracic structure and impair normal lung development, leading to restrictive respiratory dysfunction in severe or progressive cases. Non-surgical management strategies are increasingly emphasized to control spinal curvature and support pulmonary function during growth. This mini review aimed to examine current evidence on non-surgical management strategies for scoliosis in pediatric complex cases and to explore their potential role in improving respiratory function and overall pulmonary outcomes.
Methods: A literature search was conducted using several scientific databases, including Google Scholar, Web of Science, PubMed, Springer, Frontiers in, Elsevier, and Scopus. The search employed key terms such as pediatric scoliosis, conservative treatment, respiratory function, and pulmonary outcomes. Studies published in English up to 2025 were included. Conference abstracts, articles without available full text, and publications written in languages other than English were excluded. Additionally, the reference lists of the selected articles were manually reviewed to identify further relevant studies.
Results: The results of the literature study show that non-surgical interventions, including bracing and scoliosis-specific exercises, effectively slow curve progression and improve thoracic mobility. These strategies also support respiratory function and may reduce the need for surgical intervention in pediatric complex scoliosis cases.
Conclusion: We concluded that non-surgical management strategies for pediatric scoliosis play an important role in improving respiratory function by addressing spinal deformity and promoting better thoracic mobility. These approaches represent a valuable therapeutic pathway for optimizing pulmonary outcomes in children with complex scoliosis conditions.
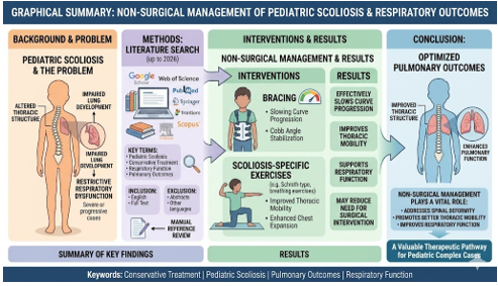
Graphical abstract: showing the different sources of searching and conclusion for the finally results of the several literatures under study.
In medically complex pediatric populations such as children with neuromuscular disorders, syndromic conditions, or spinal cord injuries the prevalence can be significantly higher due to underlying neuromuscular weakness, impaired postural control, and systemic comorbidities (Cunha et al., 2023). These children often experience earlier onset and more rapid progression of spinal deformities, making scoliosis a critical concern in pediatric rehabilitation and respiratory care (Molinares et al. 2022, Trabacca et al., 2026). Spinal deformities associated with scoliosis can significantly affect respiratory mechanics, particularly in growing children. The abnormal curvature of the spine alters the shape and flexibility of the thoracic cage, reducing chest wall compliance and limiting lung expansion. As deformity progresses, these structural changes can lead to decreased lung volumes, impaired ventilation, and the development of restrictive lung disease. In severe cases, scoliosis may compromise gas exchange and increase the work of breathing, potentially resulting in chronic respiratory insufficiency or cardiopulmonary complications (Wang et al., 2023).
Early identification and conservative management of pediatric scoliosis are crucial to minimizing curve progression and preserving pulmonary function. Non-surgical strategies including physiotherapy, bracing, and targeted exercise programs aim to control spinal curvature while maintaining thoracic mobility and respiratory capacity during growth (Mbamalu et al., 2023). Evidence suggests that early interventions can help stabilize spinal alignment, improve posture, and support pulmonary function by preventing severe thoracic deformity. Additionally, conservative management is particularly valuable for medically complex children who may not be suitable candidates for surgical correction due to comorbidities or increased surgical risk. Therefore, timely implementation of non-surgical management strategies plays a key role in optimizing respiratory outcomes and improving overall quality of life in pediatric patients with scoliosis (Wang et al., 2025). So, the aim of our minireview was to examine the effect of non-Surgical scoliosis management pediatric on improvement of respiratory function.
Study Design
This study is a structured narrative mini-review conducted to summarize current evidence on non-surgical management strategies for pediatric scoliosis and their impact on respiratory outcomes. Although not a full systematic review, efforts were made to enhance methodological transparency and rigor.
Data Sources and Search Strategy
A comprehensive literature search was conducted across multiple electronic databases, including PubMed, Scopus, Web of Science, ScienceDirect (Elsevier), SpringerLink, Frontiers, and Google Scholar. The search covered studies published between 2012 and 2025. Search terms were developed using relevant keywords and combined using Boolean operators (AND, OR). The main search string included: pediatric scoliosis or adolescent idiopathic scoliosis, non-surgical management or conservative treatment or bracing or physiotherapy or exercise therapy and respiratory function or pulmonary outcomes or Forced Vital Capacity (FVC) or Forced Expiratory Volume (FEV1) or Total Lung Capacity (TLC). Additionally, manual screening of reference lists of included studies was performed to identify further relevant publications.
Study Selection Process
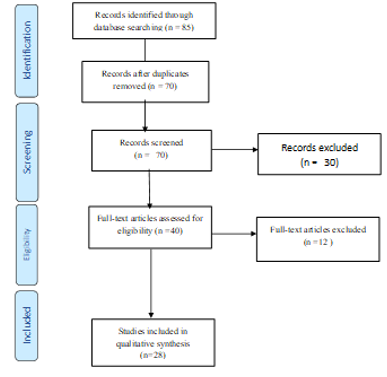
The initial search yielded approximately 85 studies. After removal of duplicates, 70 studies remained and were screened based on title and abstract. Of these, 40 articles were assessed for full-text eligibility. Finally, 28 studies were included in the review based on relevance to the topic and inclusion criteria. A simplified PRISMA flow diagram was constructed to illustrate the study identification, screening, eligibility, and inclusion process Figure 1.
Eligibility Criteria
Studies were included if they were published in peer-reviewed journals, were written in English, focused on pediatric scoliosis, investigated non-surgical management strategies and reported respiratory or pulmonary outcomes. While studies were excluded if they focused solely on surgical interventions, did not assess respiratory outcomes, were conference abstracts, editorials, or non-English publications and had no accessible full text.
Data Extraction and Synthesis
Relevant data were extracted from the included studies, including study design, population characteristics, type of intervention, and reported respiratory outcomes (e.g., FVC, FEV1, TLC). The findings were synthesized narratively to highlight trends, consistencies, and variations across studies.
Quality Considerations
Although formal quality scoring was not performed, priority was given to recent studies, systematic reviews, randomized controlled trials, and publications from high-impact peer-reviewed journals to ensure the reliability of the included evidence.
Scoliosis
Scoliosis is a three-dimensional (3D) spinal deformation characterized by lateral curvature across one or more segments of the spine, combined with vertebral rotation, which causes core deviation and sagittal advancement (Lacroix et al., 2023). Severe scoliosis can cause serious health problems such as cardiovascular disease, impaired pulmonary function, persistent pain, and psychological discomfort. There are three types of scoliosis: idiopathic, congenital, and neuromuscular. The most prevalent type, adolescent idiopathic scoliosis (AIS), has an unclear origin, as indicated by the word "idiopathic" (Peng et al., 2020). Idiopathic scoliosis can be grouped into age brackets based on when it appears. Infantile (ages 0-3 years), Juvenile (ages 3-10 years), Adolescent (ages 10-18 years), and Adult (beyond the age of 18). AIS is most recognized in childhood and adolescence, particularly during periods of fast growth. In more severe situations, treatment options include observation, the use of orthotic braces, and surgery (Applebaum et al., 2020). Congenital scoliosis results from aberrant spine development during the embryonic stage, which might include vertebral no segmentation, irregular form, or abnormal amount. This type of scoliosis is frequently connected with genetic factors and may coexist with other congenital anomalies; thus, it is typically diagnosed at birth or in early infancy. Surgical correction is the primary treatment approach, particularly for severe or fast increasing curvature (Li et al., 2024).
Prevalence of scoliosis in children and adolescents
The occurrence of scoliosis is mostly determined by the Cobb angel cut-off level. Even at the SRS's suggested 10° cut off, the incidence varies greatly over the world. It ranges between 0.13 and 2.52% among schoolchildren aged 6 to 17 (Rüwald et al., 2020; Wang et al., 2025). Congenital scoliosis is the most prevalent spinal abnormality in neonates, affecting one in every 1000 live births and with an estimated global frequency of 1% to 4% (Walters et al., 2024). Depending on the type of defect, vertebral abnormalities may be silent or unnoticeable until they are accidentally discovered. Congenital vertebral abnormalities may occur alone but are linked with other anatomical defects in up to 61% of cases (Mackel et al., 2018). Scoliosis is a common component of a variety of neuromuscular illnesses and is treated accordingly based on the underlying pathogenic reasons. The highest prevalence of neuromuscular scoliosis is found in children with medullary lesions, when curvatures occur in all cases. Next, Duchenne muscular dystrophy and Friedreich ataxia had scoliosis rates of 90% and 80%, respectively (Blevins et al., 2018). Idiopathic scoliosis makes up about 75% to 80% of all scoliosis cases. Idiopathic scoliosis can be classified further based on when it first appears infantile, juvenile, or adolescent. Juvenile idiopathic scoliosis accounts for around 10% of all idiopathic instances and develops between the ages of 4 and the first decade of life (Grabala, 2019). Adolescent idiopathic scoliosis (AIS) is the final variety, which occurs in older children and young adults and accounts for over 90% of all idiopathic instances. It occurs after the first decade of life and continues until the age of 18. The current estimated global prevalence of AIS ranges from 0.47 to 5.2% (Addai et al., 2020; Aulia et al., 2023). Gender has a substantial impact on scoliosis incidence and progression. Substantial research has repeatedly shown that scoliosis affects girls more than males. A meta-analysis found that females have a significantly higher prevalence of scoliosis, with a pooled prevalence rate of 4.06% versus 2.58% in males. This disparity is more pronounced throughout adolescence, when scoliosis is most likely to develop. Estrogen impacts may be a major contributor to this greater incidence in females. During puberty, higher estrogen levels in females may alter the spinal column growth and development (Li et al., 2024).
Classification and pathological pathways of Scoliosis. Scoliosis can be characterized according to its cause, such as idiopathic (primary) or secondary. Idiopathic scoliosis is classified into subtypes based on the age of onset, such as infantile, juvenile, and adolescent, or early and late onset. Other underlying medical issues that can cause it include congenital abnormalities, neuromuscular conditions, tumors, trauma, and syndromic conditions. Scoliosis can also be characterized based on the side of the curvature, which is either left or right. Scoliosis curves are further characterized based on the apical vertebral level (Irianto and Yazid, 2019). The different types of scoliosis are as follows:
1) Idiopathic scoliosis
Idiopathic scoliosis is a three-dimensional anatomical deformity that requires careful consideration in all planes of the body. The lateral curvature, visible in the coronal plane, produces the characteristic S-shaped truncal deformity in affected children. Additionally, idiopathic scoliosis involves a significant rotational component in the axial plane, which is often underrecognized. This rotational deformity becomes apparent during the forward bend test as a rib cage prominence or hump. Multiple theories have been proposed to explain the structural origin of idiopathic scoliosis, including biomechanical defects, neurological factors, hormonal influences, and environmental contributions (Fadzan and Bettany-Saltikov, 2017). Vertebral growth occurs at the epiphyses located at the superior and inferior poles of the vertebral bodies. Pressure differences within the intervertebral spaces lead to asymmetric growth, causing some regions to progress more rapidly or slowly than others. These pressure variations may have a genetic basis or result from the surrounding soft tissue network that supports the developing spine. Other theories suggest that imbalances in the paravertebral musculature are a major contributing factor. Numerous studies have identified differences in muscle activity, neuronal control of stabilizing muscles, and variations in skeletal muscle fiber composition along the spine. Hormonal differences may also partially explain the higher prevalence of AIS in females (Grivas et al., 2016). As illustrated in Figure 2, the interplay of these factors collectively produces the characteristic three-dimensional deformity observed in idiopathic scoliosis.
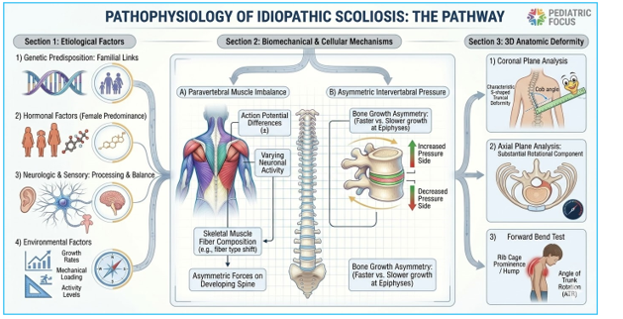
Figure 2: The complete physiological pathway of idiopathic scoliosis from cause to deformity.
• Congenital scoliosis
Congenital scoliosis is present at birth, although the spinal curves may not become apparent for several years. Many cases are attributed to genetic mutations in the HOX gene group. Congenital scoliosis is classified into three main types: failure of formation, failure of segmentation, and mixed anomalies. Each type is further subdivided according to the anatomical location of the defect. This classification aids in predicting the natural progression of the curves (Wise et al., 2020). Generally, failures of segmentation have a more favorable prognosis compared to failures of formation and mixed anomalies. Outcomes are typically poorer for anomalies located in junctional regions, such as the thoracolumbar junction. These curves are frequently associated with neurological, cardiac, and urinary abnormalities and are often detected through prenatal ultrasound (Haleem and Nnadi, 2018).
The etiology of congenital scoliosis originates from an embryologic insult occurring between the fourth and eighth weeks of gestation. Vertebral development begins with the precartilage stage (week 4), during which mesenchymal cells migrate to form a column that serves as the foundation for vertebral bodies (Mehmood et al., 2024). By week 6, the chondrification stage commences, leading to the formation of cartilaginous centrums, which subsequently give rise to the spinous and transverse processes. The final ossification stage begins thereafter and continues until approximately 25 years of age, underscoring the complexity and extended duration of vertebral column maturation. During this critical gestational window, the embryo undergoes spinal component formation and segmentation, rendering it highly susceptible to teratogenic influences due to the concurrent development of the neural tube (Blevins et al., 2018). As illustrated in Figure 3, the timeline of vertebral column development highlights the stages at which disruptions may result in congenital scoliosis, emphasizing the importance of early detection and a thorough understanding of developmental pathophysiology.
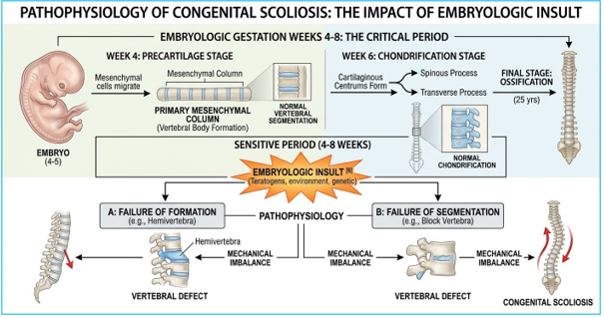
Figure 3: A Visual Timeline of Vertebral Column Development and the Pathophysiology of Congenital Scoliosis.
• Infantile and juvenile scoliosis
Spinal curves that develop in children between the ages of 0–3 years and 4–10 years are classified as infantile and juvenile idiopathic scoliosis, respectively. More recently, curves manifesting before the age of 10 have been collectively termed “early-onset scoliosis.” Children with an earlier onset of the deformity are at a higher risk of lower respiratory system impairment, which may adversely affect life expectancy. The risk of respiratory complications is commonly assessed by measuring the rib-vertebral angle difference (RVAD) in relation to the Cobb angle (Yoshida et al., 2018).
• Adolescent scoliosis
Adolescent idiopathic scoliosis (AIS) is the most common form of scoliosis, accounting for approximately 80% of cases. The incidence of mild curves is similar in both sexes; however, larger curves are more frequently observed in females. These curves often become noticeable when the deformity progresses to the point that asymmetry in the shoulders, waist, or back is apparent to others. The risk of curve progression in AIS can be predicted by several factors, including the initial magnitude of the curve at presentation, the presence of double curves, and the rate of growth during the adolescent growth spurt. Additionally, premenarchal status and skeletal immaturity, as assessed by the Risser grade, are associated with an increased potential for curve progression (Lenz et al., 2021).
2) Neuromuscular scoliosis
Neuromuscular scoliosis is a type of scoliosis resulting from neurological or muscular conditions that compromise the normal alignment and support of the spine. Historically, poliomyelitis was the primary cause of this form of scoliosis; however, currently, the most common causes are cerebral palsy and spina bifida. This type of scoliosis also occurs in progressive neuromuscular disorders such as Duchenne muscular dystrophy and spinal muscular atrophy (Dimitrakis and Zafeiris, 2023). Children with neuromuscular scoliosis typically present with difficulties in muscle coordination and sitting rather than with pain. As trunk muscles weaken, the spine gradually collapses, producing a long, C-shaped curve. These curves are often progressive and tend to worsen during periods of rapid growth, such as puberty, particularly in children with severe cerebral palsy (Wishart and Kivlehan, 2021).
The Scoliosis Research Society classifies neuromuscular scoliosis into neuropathic and myopathic forms. It is generally believed to result from insufficiency in upper or lower motor neurons, leading to weakness of the spinal stabilizing muscles (Lloyd et al., 2025). Although an underlying neuromuscular disorder or injury is present, the exact pathophysiology remains incompletely understood. Loss of muscle tone or sensory feedback along the spinal nervous tract causes biomechanical imbalances, which contribute to spinal deformity. In conditions such as cerebral palsy and myelodysplasia, asymmetric paraplegia is common, resulting in uneven forces acting on the spine (Blevins et al., 2018).
Imbalanced tone in the paraspinal musculature facilitates the rapid development and progression of spinal curvatures. Similarly, hip girdle muscle imbalances may produce pelvic obliquity, which can induce compensatory curves in the coronal plane. Additionally, selective dorsal rhizotomy; a procedure that removes abnormal sensory nerve fibers transmitting information from skeletal muscle to the spinal cord used to manage spasticity in cerebral palsy patients, can contribute to spinal deformity (Gurd and Badve, 2020). The biomechanical consequences of reduced muscle tone or altered sensory input along the spinal nervous tract create muscular imbalances that drive deformity, as illustrated in the pathophysiologic cascade in Figure 4.
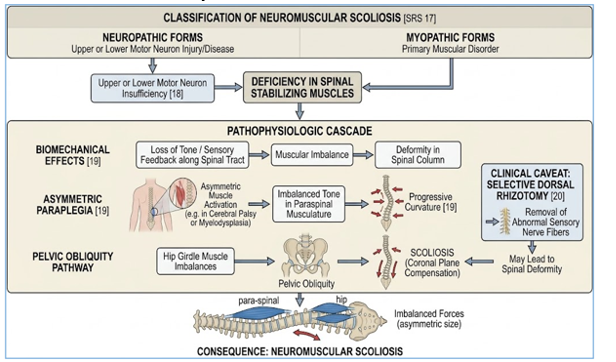
Figure 4: The Pathophysiology of Neuromuscular Scoliosis. A Biomechanical Cascading Model
3) Developmental or syndromic scoliosis
Syndromic scoliosis refers to a form of scoliosis associated with various genetic or systemic syndromes, including skeletal dysplasia, connective tissue disorders, and neuromuscular conditions. Common syndromes linked to scoliosis include neurofibromatosis, Marfan syndrome, Rett syndrome, Prader-Willi syndrome, osteogenesis imperfecta, and Ehlers-Danlos syndrome. Children with syndromic scoliosis generally face a higher risk of medical complications and surgical challenges compared to those with idiopathic scoliosis (Ballhause et al., 2019).
Diagnosis of scoliosis
Early diagnosis of scoliosis offers the advantage of implementing preventive measures, and in certain cases, treatment may be limited to conservative approaches. Screening for idiopathic scoliosis is a valuable and feasible strategy to reduce the need for surgical interventions and associated complications, as bracing has been shown to effectively prevent curve progression in most early-stage cases (Studer and Hasler, 2024). A comprehensive evaluation should include birth and family history, as well as a thorough physical examination assessing height and weight, skin stigmata, lower limb anomalies, dysmorphic facial features, shoulder and pelvic asymmetry, truncal balance, scapular prominence, curve flexibility, thoracic kyphosis, lumbar lordosis, range of motion, gait pattern, and a complete neurological assessment (Irianto and Yazid, 2019).
In younger children, the spine can be evaluated while the child is suspended to assess flexibility and pelvic obliquity, as well as during everyday activities such as walking and squatting. Lower extremities should always be checked for deformities or length discrepancies. Scoliosis typically consists of a primary and secondary curve, each with convex and concave sides. The primary curve is usually more rigid, and its location in the cervical, thoracic, or lumbar region is determined by the vertebral apex in the coronal plane (Haleem and Nnadi, 2018). A junctional curve forms where two spinal regions converge. The end vertebrae are the most cephalad and caudal vertebrae with surfaces inclined toward the concavity of the curve, and the apical vertebra is the most rotated within the curve. Curve magnitude is measured using the Cobb angle, usually expressed toward the concavity. The Cobb angle is essential for evaluating the initial curve, monitoring progression, and determining the optimal timing for surgical intervention. Unlike the previously used Cobbometer, modern measurements can be performed with computer-assisted software (Trac et al., 2019). In young children, the Adams forward bending test used to detect rib prominence in the thoracic spine or transverse process prominence in the lumbar spine may not always be feasible (Rusnák et al., 2019). In such cases, the test can be simulated by placing the child prone on the examiner’s knees. Curve flexibility can also be assessed with the child in a lateral position on the examiner’s knees or supported on the examiner’s arm. Coronal and sagittal spinal balance should be evaluated, including truncal alignment, head tilt, shoulder asymmetry, and pelvic balance. A thorough neurological examination assessing motor, sensory, and reflex functions including abdominal reflexes should be performed (Salandy et al., 2019).
Treatment of pediatric scoliosis
The treatment of pediatric scoliosis depends on the etiology, curve magnitude, and remaining growth potential. The primary goal of management is to achieve skeletal maturity with a balanced spine that is unlikely to progress further. Curves exceeding 40–50° at skeletal maturity are generally expected to continue progressing. Treatment strategies should prioritize the least invasive approach that can effectively achieve these objectives for each individual patient. Management of pediatric scoliosis is broadly categorized into non-surgical and surgical approaches (Parr and Askin, 2020).
Non-surgical Treatment
Non-surgical treatments, including bracing, exercise therapy, chiropractic care, electrical stimulation, and observation, remain the first-line approaches for managing scoliosis, particularly in cases with mild to moderate curves. In recent years, the use of wearable devices for both the diagnosis and management of scoliosis has been expanding (Caviedes et al., 2020). These devices, equipped with sensors, are designed to monitor human activity and physiological parameters in real time. In scoliosis management, wearable systems enable continuous monitoring of spinal motion and posture, facilitate remote rehabilitation, provide biofeedback, and support individualized treatment strategies (Fazeli Veisari et al., 2025).
• Braces
Management and treatment decisions need to be considered individually for every patient. For curves of less than 25 degrees, observation is usually recommended. The 2016 Scoliosis Orthopedic and Rehabilitation Treatment (SOSORT) guidelines advise against bracing for curves below 15°±5° (unless justified and carried out by an experienced physician). Bracing is recommended full time (>18h/day) for all types of idiopathic scoliosis during growth for curves above 20°±5°Cobb. Casting (very rigid bracing) is only applied for IIS or to treat curves between 45–60°Cobb inane fort to avoid surgery (Negrini et al., 2018). Braces can be worn full-time (18–23/24h) or part-time (12h, mainly at home and at night). Two of the main factors for bracing success are wearing time and curve reduction in the brace (Capek et al., 2022). Thus, part-time application of a highly corrective brace is well suited for relatively mild and supple scoliosis, allowing normal involvement in sport, social and school activities. Avoiding impairment of quality of life by full-time use helps treatment acceptance and compliance. In severe scoliosis (>35 - 40◦) or in case of progression under part-time bracing a full-time brace is needed. The most widely used in France are the Chˆeneau-Toulouse-Munster (CTM) and Lyon braces (Figure 4), (Wang et al., 2021; De Chelle et al., 2022).

Figure (4): Photographs of various types of braces (Angelliaume et al., 2025).
The indications for treatment with bracing are generally curves of 20–40° in a growing child, with age at 15 years or younger and skeletal immaturity (Risser 0–3). Observation follow-up intervals of 3 to 6 months, depending on the curve magnitude and the remaining growth potential, should be maintained to check for signs of curve progression. Significant curve progression is defined as a 5–10 degree increases within 6 months (more than 1° per month) or 10 degrees within 12 months (Kaelin, 2020). In these cases, as well as in cases of skeletally very immature patients (Risser 0; Tanner 1–2) earlier intervention with bracing in patients with curves under 25° are war ranted. These efforts are made to prevent an increase of the curve to greater that 30° at skeletal maturity, due to their progressive nature during later adult life, and to prevent surgery. Proper bracing regimens may be very effective, as for example with timely initiation JIS has been shown to be successfully treatable this way. With good patient compliance, bracing can significantly reduce curve progression (Verhofste et al., 2020). A range of scoliosis braces have been developed over the years, including rigid thoracolumbosacral orthoses (TLSO), dynamic braces that allow some movement while applying corrective forces and night-time-only braces designed to be worn during sleep (Karimi and Rabczuk, 2018). These braces are typically custom-fitted and prescribed with specific usage protocols by clinicians. The advantages of bracing and other non-surgical interventions are substantial. When prescribed and used appropriately, they can delay the need for surgery until skeletal maturity or, in many cases, avoid surgical intervention altogether. Bracing has also been associated with psychosocial benefits, such as reduced anxiety around future surgery, and physiological benefits, including improved postural control and spinal alignment during growth (Luca et al., 2020; Selthafner et al., 2021).
• Exercise therapy
Exercise therapy can slow the progression of scoliosis in patients with adolescent idiopathic scoliosis (AIS), improve spinal motor control, and enhance cardiopulmonary function. Additionally, it has positive effects on psychological well-being, helping to alleviate symptoms of depression and anxiety (Yagci and Yakut, 2019). Exercise therapy is widely recognized by researchers and the medical community due to its specific therapeutic effects, high feasibility, strong patient adherence, minimal side effects, and cost-effectiveness. Studies have demonstrated that exercise therapy is an essential intervention for patients with mild AIS to prevent progression to surgical criteria and serves as a supplementary approach for patients with severe scoliosis (Romano et al., 2012). Common examples of exercise therapy for scoliosis include:
Schroth Methodology (Germany): This widely used and studied approach incorporates the proprietary Schroth Rotational Angular Breathing (RAB) technique. It is a three-dimensional scoliosis treatment that emphasizes patterned postural correction based on the Schroth classification (Moramarco and Borysov, 2017).
Core Stabilization Exercises: These exercises strengthen the core muscles and enhance the strength of deep and superficial muscles along the spine, promoting vertebral stability. They enable patients to maintain spinal balance and torso control both at rest and during movement (Yildirim et al., 2022).
Lyon Therapy (France): This approach focuses on maintaining proper spinal alignment during exercise, emphasizing lumbar lordosis and thoracic kyphosis. It includes frontal segmental mobilization, plane correction, proprioception, core stabilization, and balance training (Ma et al., 2024).
Scientific Exercise Approach to Scoliosis (SEAS, Italy): SEAS emphasizes autocorrection and stabilization. Exercises are tailored to address deficits identified during the initial evaluation, such as muscle weakness, tightness, or impaired motor coordination (Romano et al., 2015).
Side Shift Method (UK): This active self-correcting technique involves intensive trunk flexion training. Patients are instructed to laterally shift their trunk over the pelvis in the direction opposite the cvexity of the primary curve (Ma et al., 2024).
DoboMed Technique (Poland): DoboMed focuses on enhancing thoracic kyphosis through closed kinematic chain exercises. The pelvis and shoulder girdle are placed symmetrically, and the corrected posture is actively stabilized to establish it as habitual (Szurmik et al., 2024). Physiotherapeutic Scoliosis-Specific Exercises (PSSE) and Core Stabilization: Developed and utilized worldwide, PSSE primarily aims to delay or slow curve progression. Preventing progression is critical to reducing the need for bracing, surgery, or both (Karavidas et al., 2024).
• Electrical stimulation
Electrical stimulation has been investigated as a conservative therapeutic option in the management of pediatric scoliosis, particularly for children who are not candidates for surgical intervention or those with underlying neuromuscular conditions. Electrical muscle stimulation aims to activate the paraspinal muscles through controlled electrical impulses, with the goal of improving muscular balance and promoting spinal alignment (Yan and Vassar, 2021). A recent study evaluated the effects of transcutaneous electrical stimulation (TES) applied to the paraspinal muscles, with concurrent monitoring of muscle activity using electromyography (EMG). The findings demonstrated that electrical stimulation can modify the mechanical response of spinal musculature and produce measurable, albeit modest, changes in vertebral alignment during movement tasks. These results support the hypothesis that paraspinal muscles play an active biomechanical role in scoliosis progression and suggest that targeted electrical stimulation may contribute to improved spinal stability and optimized muscle activation patterns (Wong et al., 2024).
Surgical treatment
Surgical intervention is indicated in severe cases of scoliosis or when conservative treatments, such as bracing, fail to prevent curve progression. Traditional surgical approaches include posterior spinal fusion and anterior spinal fusion, which utilize rods and screws to correct spinal deformity and achieve stabilization. In recent years, advancements in minimally invasive surgical techniques and navigation systems have significantly reduced surgical trauma and complication rates while improving the accuracy and safety of these procedures (Kuang et al., 2025). Furthermore, newer surgical strategies, such as growth rods and vertebral body tethering, have expanded treatment options for patients with remaining skeletal growth. Evidence suggests that surgical management can lead to substantial improvements in spinal alignment and functional outcomes. However, postoperative rehabilitation and long-term follow-up remain essential to ensure optimal patient outcomes and maintain correction over time (Senkoylu et al., 2020).
Effects of Scoliosis on the Breathing Pattern
In the absence of underlying disorders, mild to moderate scoliosis (i.e., Cobb angle <70>100°), patients are at increased risk of developing chronic respiratory failure and pulmonary hypertension, often resulting from chronic atelectasis, hypoxemia, and hypercapnia (Li et al., 2022). A schematic summary of these pathophysiological mechanisms is presented in Figure 5.
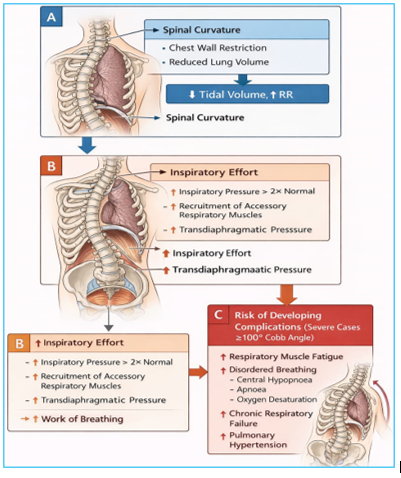
Figure 5: Pathophysiological mechanisms of respiratory dysfunction in scoliosis. (A): Spinal curvature leads to chest wall restriction and asymmetric thoracic expansion, resulting in reduced lung aeration. Consequently, tidal volume decreases and respiratory rate increase to maintain ventilation. (B): Compensatory mechanisms include increased inspiratory pressure and transdiaphragmatic pressure with greater recruitment of rib cage and abdominal muscles, which assist ventilation but significantly increase the work of breathing. (C): The increased work of breathing predisposes patients to respiratory muscle fatigue and disordered breathing during sleep, including central hypopnoea and apnoea with oxygen desaturation. In severe cases, this may progress to chronic respiratory failure and pulmonary hypertension.
Non-Surgical Scoliosis Management and Respiratory Function
Scoliosis reduces the compliance of both the chest wall and lungs, thereby increasing the work of breathing at rest, during physical activity, and during sleep. In severe cases, complications such as pulmonary hypertension and respiratory failure may develop (Hashem, 2025). Previous studies have demonstrated an association between thoracic spinal deformity and pulmonary impairment. Factors such as curve severity, the number of involved vertebrae, curve location, and reduced thoracic kyphosis have all been implicated in pulmonary dysfunction, although the strength of these associations varies across studies (Romberg et al., 2020). Consequently, severe scoliosis in childhood can adversely affect the development and function of the cardiopulmonary system, as well as trunk balance. Structural deformities of the spine and thoracic cage are well known to be associated with restrictive ventilatory impairment. Reduced lung function may become evident even with minimal physical exertion. Progressive stiffening of deformed tissues further limits chest wall mobility, exacerbating respiratory compromise (Bishop and Malone, 2024). In advanced cases of idiopathic scoliosis, respiratory failure may occur, necessitating assisted ventilation. However, the long-term pulmonary outcomes following surgical correction in patients with adolescent idiopathic scoliosis remain incompletely understood (Tandon et al., 2020). The impact of orthotic bracing on pulmonary function in pediatric scoliosis has also been investigated. One study assessed pulmonary parameters in adolescents with idiopathic scoliosis before and during brace use. The results demonstrated reductions in vital capacity, forced expiratory volume, and peak expiratory flow while the brace was worn, suggesting that rigid bracing may temporarily restrict thoracic expansion. Although bracing remains a cornerstone of conservative management for controlling curve progression, these findings highlight the importance of considering respiratory mechanics when designing non-surgical treatment strategies (Yagci et al., 2019). More recent research has focused on combining physiotherapeutic interventions with orthotic treatment to optimize both spinal alignment and respiratory outcomes. Studies evaluating the Schroth method a scoliosis-specific physiotherapeutic exercise program have reported improvements in pulmonary parameters, including inspiratory vital capacity, forced vital capacity, and forced expiratory volume, in patients undergoing rehabilitation. These findings suggest that targeted respiratory and postural exercises may enhance lung function and thoracic mobility, supporting the role of multidisciplinary conservative approaches in the management of pediatric scoliosis (Stein et al., 2024).
Evaluation of Respiratory Outcomes
Non-invasive rehabilitation methods, such as breathing exercises and aquatic therapy, were associated with more consistent improvements in pulmonary function. A recent systematic investigation reported in literature examined the influence of scoliosis treatment strategies on pulmonary function across both immediate and long-term follow-up periods. It explored differences between conservative and surgical interventions and emphasized several contributing factors that may affect respiratory outcomes in individuals with scoliosis. This systematic review focused on forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1) and total lung capacity (TLC), (Hashem, 2025). The analysis of other respiratory outcomes across various studies revealed a diverse range of results, emphasizing both improvements and challenges in pulmonary function measures following intervention. Several studies on breathing and exercise interventions have shown improvements in pulmonary function. Kumar (2024) demonstrated that both breathing exercises and conventional exercise therapy led to increases in FVC, FEV1, and PEF, with conventional exercise proving slightly more effective. A breathing exercise protocol significantly improved pulmonary function, with FVC increasing by 1.59 L, FEV1 by 1.48 L, and PEF by 3.77 L/s. Additionally, the study found that the FEV1/FVC ratio changed by 85.12% and the VC improved by 1.78 L. On the other hand, conventional exercise therapy showed similarly promising results, with FVC increasing by 1.81 L, FEV1 by 1.66 L, and PEF by 4.11 L/s. The FEV1/FVC ratio improved by 81.32% and the VC increased by 2.06 L. These results suggested that both exercise regimens were effective in enhancing pulmonary function, with the conventional therapy showing slightly superior improvements in most parameters. Ogonowska-Slodownik et al. (2020) found that aquatic breathing improved lung function, whereas corrective swimming had a negative effect. They found that the aquatic breathing program increased the FVC from 3.54 L to 3.61 L and the FEV1 from 2.88 L to 3.05 L. They also found that corrective swimming led to decreases in both the FVC and FEV1, indicating that different types of aquatic exercise might have varying impacts on pulmonary function. Küçük et al. (2024) noted that spinal mobilization combined with core stabilization exercises significantly improved FVC, FEV1, and PEF, whereas core stabilization alone had a moderate impact. Amăricăi et al. (2020) also showed that a rehabilitation program led to improvements in FVC, FEV1, and PEF, although the FEV1/FVC ratio showed only slight gains. Finally, the literature indicates that non-surgical management strategies for pediatric scoliosis are effective in controlling curve progression and supporting respiratory function. Bracing remains the primary conservative intervention, particularly for curves between 20° and 40° in growing children and can significantly reduce progression when worn according to prescribed schedules.
Physiotherapeutic scoliosis-specific exercises (PSSE), including the Schroth, SEAS, Lyon, Side Shift, and DoboMed methods, have been shown to improve thoracic mobility, inspiratory vital capacity, and overall cardiopulmonary function. Electrical stimulation may provide additional benefits in enhancing paraspinal muscle activation and spinal stability, especially in neuromuscular scoliosis, although evidence is limited. Chiropractic care has demonstrated modest improvements in Cobb angles and patient comfort in mild-to-moderate idiopathic scoliosis. Studies highlight that non-surgical interventions are most effective when initiated early, individualized, and combined in a multidisciplinary approach, with continuous monitoring of spinal and respiratory parameters. Despite these benefits, rigid bracing may temporarily restrict thoracic expansion, suggesting that respiratory function should be considered when designing treatment protocols. Overall, conservative management shows promise in preserving pulmonary outcomes and delaying or avoiding the need for surgical intervention in pediatric complex scoliosis cases.
Findings of the Studies
The studies summarized in Table 1 indicated that combined therapy, consisting of bracing and physiotherapeutic scoliosis-specific exercises (PSSE), consistently demonstrates the highest effectiveness in preventing curve progression among pediatric and adolescent patients with idiopathic scoliosis. PSSE alone, while sometimes less effective in structural correction, has been shown to improve quality of life, self-image, and respiratory outcomes. In contrast, bracing alone may restrict pulmonary function, particularly forced vital capacity and total lung capacity. Notably, some studies reported limited benefits of PSSE, highlighting variability due to curve severity, skeletal maturity, and patient adherence.
| Author (Year) | Population | Intervention | Outcomes | |
| Ma et al., (2023) | Children and adolescents with idiopathic scoliosis | PSSE | PSSE was superior to general exercise and conventional therapies in reducing Cobb angle. While not superior to bracing in curve correction, it significantly improved quality of life, including pain, self-image, and mental health. It demonstrated a faster onset and was effective in slowing progression, particularly in mild cases. | |
| Karavidas & Tzatzaliaris, (2022) | Adolescents with AIS (n = 95) | Bracing + PSSE | Combined treatment achieved an 88.5% success rate in preventing curve progression. Only 6.4% exceeded 40° and 1.1% exceeded 50°. Improvements were also observed in aesthetics, trunk rotation, mental health, and function. | |
| Zhang et al., (2023) | AIS patients (40–60° curves) refusing surgery | Intensive bracing + PSSE | Treatment was effective in 78% of patients. Larger baseline curve, lower Risser stage, and smaller in-brace correction were associated with treatment failure. | |
| Badowska et al., (2024) | Girls with AIS | Chêneau brace + Schroth exercises | Long-term treatment resulted in reduced VC, FVC, and FEV1, but increased inspiratory muscle strength (PImax). Expiratory muscle strength did not change significantly. | |
| Stanaj et al., (2025) | Adolescents with moderate AIS | Rigid bracing vs. Schroth + bracing | Bracing alone reduced pulmonary function (FVC, FEV1, TLC), whereas combined therapy improved IVC (+2.56%), FVC (+3.99%), and FEV1 (+2.36%). | |
| Liu et al., (2023) | Patients with severe AIS | Schroth vs. aerobic exercise | Schroth exercises significantly improved pulmonary function, walking distance (6MWT), and reduced fatigue (Borg scale) compared to aerobic exercise. | |
| Satanovsky et al., (2025) | Patients with neuromuscular scoliosis (myopathy) | Surgical vs. non-surgical management | Despite risks, surgical scoliosis correction improved quality of life. Note: not directly related to non-surgical pediatric AIS. | |
| Jia et al., (2025) | 1,014 patients with AIS | PSSE | PSSE significantly improved Cobb angle, ATR, and quality of life. | |
| Ren et al., (2025) | Patients with AIS (multiple RCTs) | Bracing vs. PSSE vs. combined therapy | Combined therapy was the most effective; individual interventions showed variable and less consistent outcomes. | |
| Baumann et al., (2024) | patients with AIS | PSSE | PSSE may not provide any clinically significant improvements in Cobb angle, ATR, or SRS-22 scores in patients with AIS. PSSE did not significantly improve Cobb angle when stratified by curve size. | |
| Jiménez-Jiménez et al., (2025) | AIS patients | Schroth method ± another conservative | Schroth method proved effective in reducing the Cobb angle and ATR, particularly in patients with mild curves and in early stages of skeletal growth. Improvements were also observed in health-related quality of life and aesthetic perception, and to a lesser extent, in pulmonary function. | |
| Abdelaal et al. (2017) | 73 adolescents with mild AIS (10–17 yrs) | Observational (no surgery; baseline respiratory assessment) | AIS patients showed significantly reduced FVC, FEV1, MVV, and 6MWT vs controls Early pulmonary impairment even in mild cases | |
| Hashem (2025) | AIS patients (systematic review) | Non-surgical therapies (breathing exercises, aquatic therapy) | Conservative interventions showed more consistent improvement in FVC, FEV1, and PEF vs variable surgical outcomes | |
| Çetinkaya et al. (2024) | 60 adolescents with AIS (20°–66°) | Brace use + respiratory muscle assessment | Respiratory muscle strength correlated with Cobb angle severity and brace duration, affecting pulmonary function | |
| Yurt et al. (2021) | 15 adolescents with AIS (~25° Cobb) | Thoracolumbosacral brace (8-month follow-up) | Brace caused temporary reduction in FVC, FEV1, PEF when worn, but no long-term deterioration in pulmonary function | |
| Di Maria et al. (2021) | Adolescents with AIS | Sforzesco brace (short-term effect) | Immediate reduction in lung volumes (VC, TLC) during brace wear, but not linked to permanent dysfunction | |
| Ran et al. (2016) | 237 AIS patients | Preoperative brace vs no brace (retrospective) | Brace group showed lower FEV1 and FVC%, suggesting possible restrictive effects depending on duration/intensity | |
| Ersen et al. (2013) | 76 AIS adolescents | SpineCor dynamic brace | Brace showed changes in pulmonary function parameters, highlighting need for monitoring during conservative treatment | |
| Basbug et al. (2023) | 36 adolescents with mild–moderate AIS | Inspiratory muscle training | Significant improvement in respiratory muscle strength, FVC, and functional capacity after IMT. | |
| Sirayder et al. (2025) | AIS adolescents | IMT (6 weeks, RCT) | Significant improvement in lung function, functional capacity, and QoL | |
Table 1: Summary of the previous studies included in the current study.
The present review of recent literature on non-surgical management of pediatric and adolescent idiopathic scoliosis (AIS) demonstrates that combined conservative interventions, particularly bracing alongside physiotherapeutic scoliosis-specific exercises (PSSE), offer the most consistent clinical benefits. Across multiple studies, combined therapy was associated with the highest success rates in preventing curve progression. For example, Karavidas and Tzatzaliaris, (2022) reported that an integrated approach using bracing and PSSE achieved an 88.5% success rate in adolescents at peak growth, with only 6.4% of patients exceeding a 40° Cobb angle and 1.1% exceeding 50° by the end of treatment. Similarly, intensive bracing coupled with PSSE was effective in 78% of patients with larger curves who refused surgery (Zhang et al., 2023). These findings underscore the synergistic effect of mechanical correction provided by bracing and active postural and muscular reinforcement offered by targeted exercises. While PSSE alone may not always surpass bracing in terms of structural correction, several studies have emphasized its significant impact on functional outcomes and quality of life. Ma et al., (2023) demonstrated that PSSE reduced Cobb angle more effectively than general exercise or conventional therapy, while also producing meaningful improvements in pain, self-image, and mental health. Similarly, Jia et al., (2025) confirmed that PSSE alone improves Cobb angle, angle of trunk rotation (ATR), and quality of life across a large cohort of over 1,000 AIS patients. However, the effectiveness of PSSE appears to be influenced by curve magnitude, skeletal maturity, and patient adherence, as highlighted by Baumann et al., (2024) who reported minimal improvements in Cobb angle and SRS-22 scores among patients with larger curves or inconsistent engagement with exercise protocols. An important consideration in non-surgical management is the effect on pulmonary function, particularly in patients undergoing bracing. Standalone rigid bracing has been associated with reductions in forced vital capacity (FVC), forced expiratory volume in one second (FEV1), and total lung capacity (TLC), reflecting the restrictive nature of bracing on thoracic mechanics (Badowska et al., 2024; Stanaj et al., 2025). In contrast, Schroth-based PSSE, whether applied alone or in combination with bracing, has been consistently shown to improve respiratory parameters. Stanaj et al., (2025) demonstrated that combining Schroth exercises with bracing improved inspiratory vital capacity, FVC, and FEV1, while Liu et al., (2023) reported enhanced pulmonary function, greater walking distances, and lower perceived fatigue in patients performing Schroth exercises compared with aerobic exercise controls. These findings suggest that integrating structured exercise programs into conservative management is essential for mitigating brace-related pulmonary restriction and optimizing overall functional outcomes. Despite these promising results, there remains variability and inconsistency across studies. Differences in patient age, curved severity, skeletal maturity, intervention protocols, duration of follow-up, and adherence contribute to heterogeneous findings. Notably, some studies, such as Baumann et al., (2024) observed limited clinical benefit from PSSE, highlighting that exercise effectiveness may be constrained in patients with larger curves or insufficient compliance. Moreover, the quality of evidence varies, with high-level randomized controlled trials and meta-analyses providing more robust support for combined interventions (Jia et al., 2025; Ren et al., 2025) while smaller cohort studies offer useful but less generalizable insights.
Clinically, these findings have important implications for physiotherapy practice. First, early initiation of PSSE, particularly Schroth-based protocols, alongside appropriately prescribed bracing, appears critical for maximizing structural correction, functional outcomes, and quality of life. Second, patient adherence to prescribed exercise regimens is essential, as benefits are closely linked to the frequency, duration, and quality of exercise performance. Third, respiratory monitoring should be considered in patients undergoing bracing alone, and inclusion of PSSE may help mitigate potential negative effects on pulmonary function. Finally, future research should focus on large-scale, multicenter randomized controlled trials to clarify the comparative efficacy of PSSE alone, bracing alone, and combined approaches across different curve severities and stages of skeletal maturity. Long-term follow-up studies are needed to evaluate sustained effects on pulmonary function, quality of life, and functional outcomes. Additionally, further investigation into strategies to improve adherence to PSSE protocols will help optimize clinical outcomes in pediatric AIS.
Moderate evidence suggests that non-surgical interventions, including scoliosis-specific exercises, core stabilization, and orthotic bracing, may improve respiratory function in pediatric scoliosis patients. Exercise-based interventions consistently showed improvements in parameters such as FVC, FEV1, and PEF, whereas rigid bracing may temporarily restrict thoracic expansion and reduce pulmonary function. The overall evidence is heterogeneous, with varying results depending on the intervention type, severity of scoliosis, and patient compliance. These findings highlight the importance of individualized, multidisciplinary conservative management and the need for further high-quality studies to clarify long-term respiratory outcomes.
Ethics approval and consent to participate: NA
Consent for publication: The authors state that none of the work described in this study could have been influenced by any known competing financial interests or personal relationships.
Availability of data and material: Data will be made available on request.
Competing interests: no conflict of interest
Funding: No fund
Authors' contributions: Conceptualization: RRS, MMA; investigation, methodology, and data curation: SAO, and RRS; preparing original draft: MMA, and SAO; review and final editing: RRS, ME, SAO and MMA. All authors read and approved of the final manuscript.
Acknowledgements: NA
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
