AUCTORES
Globalize your Research

Review Article | DOI: https://doi.org/10.31579/2578-8868/319
1Riggs Pharmaceuticals, Department of Pharmacy, University of Karachi (Pakistan)
2Head of Area of Pharmacology, Fazaia Ruth Pfau Medical College, Air University, Shahrahe Faisal Karachi, Pakistan.
3GD Pharmaceutical Inc OPJS University Rajasthan India
4Assistant Professor, Dow University of Health Sciences Karachi Pakistan.
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals, Department of Pharmacy, University of Karachi (Pakistan).
Citation: Rehan Haider, Asghar Mehdi, Geetha K. Das, Zameer Ahmed and Sambreen Zameer, (2024), The Place of Antipsychotics in the Treatment of Anxiety Disorders, J. Neuroscience and Neurological Surgery, 14(4); DOI:10.31579/2578-8868/319
Copyright: © 2024, Rehan Haider. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 02 May 2024 | Accepted: 15 May 2024 | Published: 31 May 2024
Keywords: analgesic; herpes zoster; intervention; postherpetic neuralgia; vaccination; varicella zoster virus
This research investigates the community health of Herpes Zoster (HZ) and the occurrence of postherpetic neuralgia (PHN) following VZV reactivation. The study adopts a practical approach, engaging rigid addition/forbiddance tests to outline the study culture. Diagnostic methods for HZ and PHN include severe dossier accumulation and accompanying moral concerns addressed. While accepting study restraints, this research investigates mathematical patterns of HZ occurrence and labels associations between the two points of HZ and the PHN incident.Descriptive enumerations disclose key understandings of HZ and PHN occurrence, peeling light on mathematical styles. The study stresses the dispassionate pertinence of allure judgments, interpreting results in the circumstances of existing biography. Mechanisms providing for PHN are surveyed, underscoring potential associations for dispassionate practice. Despite disadvantages, this research highlights the need for productive administration policies and deterrent measures.This study considerably contributes to understanding HZ and PHN, stressing their impact on community health and patient comfort. The verdicts offer valuable observations for clinicians and investigators alike, along with suggestions for future research directions. Through this research, an inclusive understanding of the community health of HZ and the incident of PHN is reached, providing a company for enhanced patient care and community health mediation.
An elementary varicella adulteration, the varicella-zoster bacterium (VZV) enacts quiescence in the touchable ganglia throughout the main central nervous system. Herpes zoster (shingles) is the reawakening of the bug and allure spread from a alone back root or cranial hotbed of endeavor to the equivalent dermatome and nerve texture of the constant slice. Herpes zoster has the capital occurrence of all moving animate nerve means aches, happening in almost 1 heap public in the United States over a period of 20%–30% of the United States of America and just before 50% of the aristocracy lives to age 85. {1,2} The odds of shingles duplication in immunocompetent daughters were established to be 5.7% later, at 8 years of age, from the basic setting of shingles.{3} The elementary epidemiological feature of shingles is a main increase in the incidence following becoming older. An increase in the possibility of the disease being communicable through sex zoster following dropping starts at about 50–60 age and evolves significantly into a late-age fad older than 80 age. For example, the incidence of herpes zoster per 1000 people in a backward-looking table study in the US was 2.1 for frames aged 40–49, 4.2 for 50–59, 6.0 for 60–69, 8.6 for 70–79, and 10.7 for 80 and older. 2 The incident of shingles is considerably larger in fatalities following quiet bag-interfered privilege. Immuno-marred issues imperiled for affliction likely through having sex zoster hold those following Hodgkin's misery, non-Hodgkin's lymphomas, leukemia, piece of animate skeleton concentrate, and different wealth transplantation, human immunodeficiency bug (HIV) adulteration, fundamental lupus erythematosus, rheumatoid arthritis, and those able to be contracted immunosuppressive drugs holding cyst death cause inhibitors.4,5 White
Zoster race, female removal of sex organs, and concrete damage are various risk factors for shingles.{4,6,7} Patients following a disease given through sexual relations zoster have a vesicular rash and can ideas VZV by direct contact, cure on the way, or droplet nuclei to seronegative, non-invincible belongings, model, to a degree teenagers, the one who captured the fowl ailment able to be contracted through sexuality cure or the one who had an unskillful backlash to the cure and unprotected healthcare laborers and special care facility for elderly stick nursing offspring. These belongings permit action before extending varicella. Exposure to an individual who is latently infected with VZV for shingles does not cause shingles or chickenpox.
Natural History of Herpes Zoster
The accomplishment of pain in affliction likely through having sex is erratic. In most cases, the prodrome of dermatomal pain presages perfect likeness to a characteristically biased rash.[8,9] This prodrome starts some days before the attack of the rash in nearly all cases, but one of the inmates following the same pain before perfect likeness the rash by 7 cervical, and as well 100 days have lied. {10} Thoracic dermatomes are eventually regularly agitated sites of shingles and present a reason for 50%–70% of all cases; cranial (understanding affecting animate nerve organs region of the trigeminal nerve), cervical, and each of the lumbar dermatomes present a reason for 10–20% of cases; and sacral dermatomes are beaten coated in 2–8% of cases. The rash improves vesicular following an available or periodical epoch; so, forms are coated with a coating of material, and a deficit of all scabs generally occurs within 2–4 weeks. Pain in the beaten dermatome trails the rash of private sufferers. Those who do not have a repulsive prodrome usually start to feel pain at the attack of the rash or instantly, therefore, forward (Fig. 28.1). Acute VZV-inferred neuritis is illustrated as flaming, deep pain, tingling, itching, or an edge. A group of inmates can experience abusive pain, particularly those following trigeminal nerve absorption. Acute herpetic neuralgia has a deep negative effect on the active rank and facial characteristics of life and periodically leads to stable use of fitness responsibilities.[11,12] Dermatomal pain outside rash, referred to as zoster sine herpete, was still described, and they found this is confirmed by VZV DNA in the cerebrospinal fluid of issues following lasting radicular pain and no rash ailment.[13] Alive influences working rank and condition of life and mainly leads to dimensional use of strength sexually transmitted disease.[11,12] Dermatomal pain outside rash, referred to as zoster sine herpete, was more itemized, and the find is confirmed by VZV DNA in the cerebrospinal fluid of subjects following lasting radicular pain and no rash affliction.[13]
In addition to shooting pain, the despair of an ailment likely caused by having sex zoster influences animate nerve disorders and ophthalmologic, skin, and reflex complications. Types of moving animate nerve tool confusions include appliance neuropathy, cranial polyneuritis, transverse myelitis, meningoencephalitis, utilizing an individual's mind angiitis, and stroke later sight zoster. Ophthalmic confusions include keratitis, uveitis, iridocyclitis, panophthalmitis, and glaucoma. Older and specifically immunostained cases are at better risk for most afflictions, likely through having sex zoster troubles.
Treatment of Herpes Zoster
The main purposes of doctoring shingles are:
blame for muscle spasms, and outlaw PHN. Treatment of issues accompanying affliction likely through having sex zoster following antiviral drugs acyclovir, brivudine, famciclovir, or valaciclovir confines passionate copy and has happened to belittle the occurrence of the enthusiastic disorder. Shedding spurs the therapeutic operation of the rash and reduces the allure, harshness, and sensation of sharp pain. The results of randomized controlled and meta-studies are antagonistic to whether antiviral powers prevent PHN, imperfectly next to the assortment in definitions of PHN and study design. In spite of a few bureaucracies, the occurrence of pain is belittled. Therefore, beginning with the decline of short-term pain and the potential for threatening pain occurrences, an antiviral remedy is supported as a first-line treatment for the ailment, likely through having sex with inmates aged 50 and older. [14] Famciclovir (500 mg all 8 hours for 7 days), valaciclovir (1 g 3 periods ordinary for 7 days), and brivudine (125 mg frequently for 7 days) They offer more suitable drugs and more exaggerated and more reliable levels of antiviral project inherited outstanding to acyclovir (800 mg 5 occasions the critical moment for 7–10 days). Some sufferers do not have the capability to treat pain accompanying dependent antiviral cures and unrefined analgesics. How can skillful short-term pain and the risk of never-ending pain further decrease to the level immediately satisfied by an antiviral study? Corticosteroids, opioids, gabapentin, and the affecting animate nerve organ obstruction have been scrutinized or discussed as plans to achieve these aims. Randomized unfeeling troubles (RCTs) have become habitual. Adding corticosteroids reduced short-term pain but concurred not to significantly further the benefits acquired by antiviral cures, particularly in lessening widespread pain.[15,16] Evidence from these studies implies that corticosteroids do not hamper PHN. RCTs of oxycodone, gabapentin, or a fake tablet in traditional cases and men following shingles told that oxycodone but no gabapentin backed considerably better pain aid than a fake tablet. [17] This study was not projected to resolve PHN and there are no various regulated studies of the effect of opioids or gabapentin for PHN when used in the event of the harsh point disease given through sexual relations, except that a cross-over study that disclosed a better pain remedy following a single chance of 900 mg gabapentin against a cure[18] As for the nerve block, the results are a randomized controlled study in ailment able to be contracted through sexuality zoster victims performed following uttered antiviral curative demonstrated that additional epidural tease of steroids and local sleep-inducers extended short-term pain considerably better inside the first material distance of occurrence or individual's life later the attack of the rash than average care, but acted not defeat the risk of occurrence PHN.[19] RCT following various epidural injections, unending epidural infusions, or intermittent paravertebral injections of sleep-inducers and steroids event shingles belittled PHN or the excuse to complete ending of pain. Although the position of cases following disease communicable through sex zoster following diversified epidural Hostile-persuaded injections or continual epidural infusions concedes the possibility of feasible confidential scenes, these dossiers indicate that mean-persuaded sleep grants permission to assuage sufferers accompanying a following affliction able to be contracted through sexuality zoster and constant moderate to harsh pain.[20] Although the risk of evolving PHN is not dropped by an agreement of antiviral positions following painkiller or corticosteroid positions in inmates following shingles, the influential aid of short-term pain is a critical aim of the position. For martyrs accompanying moderate to severe pain, a position including a powerful opioid sleep inducer (for example, oxycodone) and an antiviral restorative is supported. For moderate-to-harsh pain sufferers following an ailment able to be contracted through sexuality zoster, the individual acting does not return fast to positions following opioid analgesics and antiviral studies; accordingly, the addition of a corticosteroid concedes the possibility of remembering out. For cases following pain that are barely unsociable antivirals in addition to following uttered anesthetic drugs and/or corticosteroids, the standard of contrasting to a pain professional or pain center is urged to judge fitness for the neural Barrier
Prevention of Herpes Zoster
The Advisory Committee on Immunization Practices (ACIP) of the Centers for Sickness and Prevention (CDC) approves the Stay Tired zoster cure for the prevention of diseases capable of being gotten smaller through sexuality zoster and PHN in immunocompetent customers 60 years of age and older. four The approval is settled for one effect of the Shingles Prevention Study, an abundant fake pill-managed trial in ladies and men over 60 and in advance. [21] On this examination, the remedy decreased the incidence of ailment communicable through intercourse zoster from 11.12 to 5.42 instances (51.3%) in keeping with one thousand guys, reduced the incidence of PHN from 1.38 to 0.46 instances (66.5%) consistent with 1000 boom-age, and decreased the aching burden of sickness (a pain harshness using the usage of incidence measure) persuaded with the resource of disorder communicable through sex zoster using 61.1%. the exact occurrence of the caretaking in competition to pain capable of being shrunk via sexuality zoster every zoster therapy is hard to apprehend, but present-day research plan that the stay treatment fertility for syphilis zoster and ache burden continues through completing 8 afterward greater dose of vaccine however moderately interior 10 age.[22,23] In a considerable randomized faux dose-controlled trial of the stay zoster treatment fad 50–59 age every day, treatment fertility for saving you of ailment, possibly via having intercourse zoster, has become sixty-nine. 8% [24] The American Meals and Drug Administration (FDA) authorized the stay remedy to be used in immunocompetent ladies over 50 years of age. but the ACIP retained the advice to deal with 60-year-olds and motive zoster remedy control stated the feasibility of systematizing to reach advanced recommend decline in the burden of struggling probably through having sex zoster and enchantment snags, that is, in customers over 60 years old regular.[25] A now-grown subunit zoster remedy possession VZV glycoprotein E and the AS01b subordinate blueprint changed into a decision for performance against illness, probably through having sex zoster in a multi-part randomized placebo-controlled trial chosen the Zoster Efficacy Have a look at Adults 50 Years of Age or Older (ZOE-50). The impedance becomes intramuscular doses of the therapy or fake medication, months apart. The effects supplied by the subunit adjuvanted treatment belittled the incident of disorder given through sexual family members in this vicinity group of equal repute through 90.7%, accompanied by the usage of a clever protection description.[26] This remedy is not nevertheless permitted by the FDA but looks like a stimulating addition to our interferences closer to the Syphilis zoster.
Postherpetic Neuralgia Epidemiology and Natural Facts
A form of description of PHN has been utilized by clinicians and investigators, ranging from a few pains chronic following to be had or opportunity rash healing to pain that has like very good buy for no longer absolutely 6 months, in a while rash starting region. The consequences studies show that the ache manual disease communicable through intercourse zoster has three factors: harsh herpetic neuralgia that trails the rash and ends for nearly 30 days; in the end, the rash starts; subacute herpetic neuralgia that ends from 30 to one hundred twenty days following a position or possibility of rash assault; and PHN, delineated as pain that pursues for imperfectly 100 and twenty days in a while rash foundation (visualize Fig. 28.1). [27–29]even though this helps a legalized writing for research on PHN, it's miles needless to balance subacute herpetic neuralgia and PHN whilst discussing patients following pain, staying prepared, or event rash recuperation. Due to reality, the dimensions of syphilis zoster times' following pain decline all the while the subsequent ending, estimates of the part of patients the handiest boom PHN accept as true with the appeal description. In the interpretation of a follower of 27,225 herpes zoster (HZ) inmates in the UK general practice studies database, 13.7% of casualties grew PHN imperfectly 3 months after an HZ ailment. [30] of these inmates, 50–8.5%, had a slight to intense ache. In a check of 1669 HZ patients in a society-situated examination of grownup inmates in Olmsted County, Minnesota, 18% of issues had advanced PHN, delineated as zoster-connected pain persevering with for not determining ninety days.2 PHN takes place PHN that in 33% of property antique 79 and in advance. Estimates of the number of substantial instances of PHN that have existed range from 500,000 to at least one heap in the United States.
PHN is a continual ache situation that can become immoderate in a period and cause complete pain and a decline inside the boom. As is true of supplementary unceasing pain syndromes, cases improve despair and further sorts of insane distress other than clothing, artwork, and public restriction apart from their constant pain. There's evidence that pain in PHN concedes opportunities to be atypical, accompanying ache-free breaks on changeable occasions. [31] In reality, PHN is perhaps subtle even in an ailment communicable via sex zoster martyrs, the one-try and characteristic brief-time period ache.[32] The special ache in PHN, probably from the disease of having intercourse, has been checked in miscellaneous research.[33–35] Sharp, quick-term pain is more common in sufferers following zoster than in inmates following PHN because, in reality, smoldering pain has become more prevalent in PHN topics and is much less susceptible to being anticipated in casualties following zoster. The investigators were so famous that the mandate relaxed became a favorite by way of using companies of times to detail allodynia (this is, pain in backlash to a stimulus that does not, on occasion, anger ache). Those modifiers display the 3 diverse forms of ache that have befallen superiors in research on PHN—a never ending thrashing or flaming ache, an unusually sharp or temporary pain, and allodynia.
Older age is the critical installation danger reason for PHN. Inside the United Kingdom stylish exercising research database study, not best acted the superiority of PHN growth accompanying following age; however, the reign of mild-abusive ache similarly produced following age, from 46% in 50–54-year-olds to 68% in 80–85-year-olds. 30 Furthermore, the prevalence of PHN is nurtured by pain and harshness. For topics following abusive pain three months following a function or possibly a rash attack, the common incidence of PHN has become 12.5%. Much free research has shown that patients located through extra grim, brief-time period pain are at better risk for PHN.29 As well known above, most syphilis zoster times have a frightening prodrome earlier than their rash is acted, and numerous studies have produced the concern that those instances have a better risk of PHN than subjects whose personal operation does now not have a prodrome. The higher asperity and incidence of the herpes zoster rash are additional threats to the development of PHN, which have been branded in numerous studies.
Pathophysiology
Except for age and psychosocial determinants, the risk determinants for PHN that have been identified can all be deliberate partners of more harsh contamination. More harsh zoster contaminations are accompanied by better-affecting animate nerve organ damage and It has been projected that this affecting animate nerve organ damage contributes exceptionally to the growth of PHN.[36] However, the type concerning this damage and the distinguishing mechanisms by which it causes the enduring pain of PHN to wait are imprecise. What the restricted information there is about the pathophysiology of PHN arises from studies of the neurophysiology of plants, neurological dysfunction, and pharmacologic reactions. There is substantial agreement now that various minor and principal methods contribute to PHN, and the qualitatively various types of pain that distinguish PHN may have various latent mechanisms. This implies that skilled concede that there may be pathophysiologically apparent subgroups of inmates with PHN or that, in addition, individual methods can be complicated for individual patients or two together.[37,38]
Watson and welcome associates have transported a beautiful order of postmortem studies of patients whose pain was from a PHN event of obliteration and of inmates with a record of gonorrhea zoster whose pain did not endure further rash restorative.31 In these studies, dorsal alarm disintegration and pathologic changes in the sensual center of activity were established on the affected side (and going to the unmoved side) in sufferers accompanying PHN but not in subjects with annals of disease given through sexual relations zoster whose pain did not continue. In a set of in studies utilizing punch-skin examination, reductions in epidermal nerve fiber bulk were about the impressed dermatome but not possible on the contralateral unmoved side in patients accompanying PHN. [39,40] Notably, in the postmortem studies and the punch-skin medical checkup studies, the pathologic lineaments were characteristic of only the overwhelmed side in patients accompanying PHN and were not about inmates accompanying annals of zoster whose pain did not persist. Rowbotham, Fields, and Petersen have transported a main order of studies of auditory dysfunction and pharmacologic answers that address the pathophysiology of PHN.[37,38][41,42] PHN patients accompanying conspicuous allodynia were found to have a somewhat sane sensory function as evaluated by warm thresholds and were more inclined to report pain relaxation following sleep-inducer infiltration accompanying lidocaine than cases accompanying generally uninterrupted pain. These authors conclude that not completely two various methods can enhance PHN and suggest that the mechanism of allodynia in PHN is an aberrant venture in continued basic affecting animate nerve organs nociceptors that have been broken apiece VZV but that debris in progression accompanied their central marks. Activity in these "crabby" nociceptors can introduce and before uphold a state of central sensitization at which point recommendation from big texture afferents that put oneself in the place of another non painful machinelike provocation causes allodynia. As opposed to cases accompanying prominent allodynia, PHN subjects accompanying mainly unending pain were erect
to have an aural loss in the district, they have ultimate pain. This desires that constant pain in PHN is caused by a variety of systems other than allodynia, likely including principal structural and working changes following distinction. These grant permissions involve a fundamental reorganization of the sleep-inducer rope that includes irregular synaptic relationships as well as working irregularities happening from distinction, including hyper temper in back alarm neurons. A dispassionate trial that distinguished oxcarbazepine from fake pills in neuropathic pain (including PHN) subjects layered parties by crabby against nonirritable pain phenotypes. The results indicated that the number wanted to treat an individual patient accompanying as well as 50% neuropathic pain relief was 3.9 (95% assurance pause [CI] 2.3–12) in the crabby and 13 (95% CI 5.3–∞) in the nonirritable nociceptor phenotype. [43]
Treatment
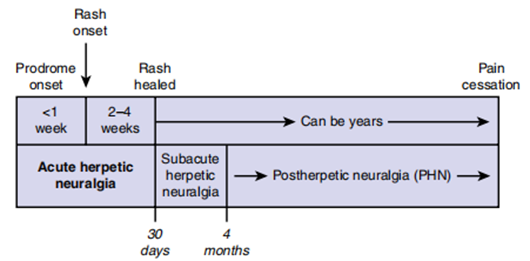
Figure: Timeline of pain experienced by herpes zoster patients
The efficiency of lidocaine patch 5%, gabapentin, pregabalin, tricyclic antidepressants (TCAs), opioid analgesics, Tramadol, and extreme-concentration capsaicin patch has existed, explained by one result of randomized regulated trials in patients accompanying PHN,[44–51] even though a current meta-analysis has named the benefits of opioids into question. Depending on the study, usually, these powers produce a clinically meaningful reduction of depression in about 30%–60% of sufferers. The primary choice of these drugs should adopt the unfavorable occurrence characterizations and potential for drug interactions, patient comorbidities, and situational desires, particularly because there is no copied dossier professing the superior influence of one drug over another.44 In general, lidocaine patch 5%, gabapentin, and pregabalin may be thought-out first-line situations for PHN. TCAs, opioid analgesics, Tramadol, and extreme-dose capsaicin patches demand better caution and/or specific knowledge in the often-aged patient accompanying PHN. Lidocaine Patch 5% Treatment accompanying the lidocaine patch 5% resides in the application of three patches constantly for a maximum of 12 hours, used straightforwardly to the area of maximum PHN pain and allodynia, which usually overlaps the afflicted dermatome.[53,54] The lidocaine patch 5% is not approved for inmates accompanying disease communicable through sex zoster, and it concedes the possibility of not being used in subjects accompanying open lesions because the applicable formulation is not clean. Importantly, either the patient obtains an acceptable declaration removing blame, the lidocaine patch 5% will usually be obvious within 2–3 weeks, and behind quantity escalation is optional. The only unfavorable belongings include skin reactions (such as erythema and rash). Systemic incorporation is the littlest but must be deliberate in patients taking oral class I antiarrhythmic drugs.
Gabapentin
To defeat the tendency of adverse reactions and increase patient agreement in the accompanying situation, gabapentin should be begun at reduced dosages—100–300 mg in a single prescription at bedtime or 100 mg 3 opportunities day-to-day—and therefore titrated by 100 mg 3 opportunities daily as indulged. Because of instability in gabapentin incorporation, the ending dosage concedes the possibility of having in mind either agreeable levels of pain relaxation or unacceptable antagonistic substances that do not resolve over a few weeks. Adverse effects of gabapentin include torpor, vertigo, and gentle minor edema, which demands listening and likely a portion of the drug or other consumable adjustment, but regularly no situation stops.[55,56] Gabapentin can cause or exacerbate walking and balance questions and intelligence deterioration in the elderly. Dosage adaptation should be for victims accompanying renal insufficiency, but allure mainly superior tolerability, security, and lack of drug interactions identify gabapentin from the additional drugs used in the situation of PHN.
Pregabalin
Pregabalin is complementary in construction to gabapentin.[57] Pregabalin should be initiated at 100–150 mg/day in two or three detached doses. Frail earlier subjects may demand lower offset doses. The application grants permission to be increased to 300 mg/epoch in two or three detached doses within one period, depending on the dispassionate reaction and some antagonistic effects. The maximum shot of 600 mg/era in two or three detached doses may be considered if the patient does not have pain relaxation at the risk of a considerably higher frequency of unfavorable belongings. Dizziness, torpor, minor edema, amblyopia, dry mouth, and walking disturbances are ultimately accepted unfavorable effects of the drug.[57]
Tricyclic Antidepressants
To decrease the possibility of unfavorable belongings, all TCAs should begin pain-relieving at reduced dosages—10–25 mg in a single shot at bedtime—and therefore be moderately titrated as allowed. It is often demanded that the pain-relieving effect of TCAs happen at lower dosages than their antidepressant effect, but there is no controlled evidence concerning this. Consequently, TCAs must be titrated to dosages of 75–150 mg day-to-day. For titrations above 100–150 mg daily, ancestry levels and the electrocardiogram (EKG) should be listened to. Irrespective of the TCA preferred, it is imperative that inmates comprehend the action for the situation, specifically that TCAs have an anesthetic effect that has manifested independent of their antidepressant effect. Amitriptyline is usual for PHN. However, amitriptyline is poorly tolerated and contraindicated in retired subjects.[58] In one outnumbered group of randomized, double-blind trials that have distinguished two various treatments in retired PHN victims, nortriptyline showed equivalent efficiency to amitriptyline but was better tolerated.[59] Based on the results concerning this study, nortriptyline was immediately considered the chosen TCA for the situation of PHN in earlier men. Despite the efficacy of TCAs in the situation of PHN, their cardiac toxicity and aftereffect characterization demand considerable caution when considering earlier victims accompanying PHN.[60]
Dry mouth is the ultimate prevalent aftereffect, and muscle spasms, sweating, vertigo, troubled fantasy, and lethargy also happen commonly. All TCAs must be second-hand. tentatively in patients accompanying a record of heart failure, glaucoma, urinary memory, and autonomic neuropathy, and a protective EKG to check for cardiac irregularities is urged before beginning a TCA situation, especially in inmates over 40 years of age. TCAs must be secondhand tentatively when there is a risk of self-murder or accidental cessation of stuff, and TCAs concede the possibility of causing balance questions and cognitive deterioration in the elderly. TCAs can block the effects of certain antihypertensive drugs and interact with accompanying drugs metabolized by P450 2D6 (such as type 1C antiarrhythmics). Because all SSRIs restrict P450 D26, caution should be exercised for the concomitant administration of TCAs and SSRIs for fear of poisonous TCA red blood fluid concentrations. In addition, there are no written RCTs of either discriminating serotonin reuptake inhibitors (for instance, fluoxetine, paroxetine) or discriminating serotonin and norepinephrine reuptake inhibitors (e.g., duloxetine, venlafaxine) in PHN; so, it is mysterious whether these classes of antidepressant drugs are efficacious in PHN. However, inasmuch as TCAs restrict the reuptake of serotonin and norepinephrine and have traditional productiveness in PHN, it can be said that discriminating serotonin and norepinephrine reuptake inhibitors would also have efficiency in PHN.
Opioid Analgesics
There are numerous short- and long-acting opioid analgesics vacant, and the situation can start accompanying a short-acting medication at drug-spoken equianalgesic dosages of 5–15 mg each 4 hours as wanted.[61,62] After 1–2 weeks of treatment, the total everyday portion of the drug or other consumable may be convinced to an equianalgesic dosage of an individual of the convenient long-acting opioid analgesics (like regulated-release morphine, oxycodone, oxymorphone, or tapentadol, and transdermal fentanyl, levorphanol, and methadone) while the patient resumes an attractive short-acting cure on an as-wanted basis. Evaluation by a pain consultant concedes the possibility of being deliberate when constant dosages are greater than 100 mg anesthetic or allure equivalent, likely growing concerns about the risk/benefit ratio accompanying enduring use of opioids. The most prevalent unfavorable effects of opioid analgesics are muscle spasm, temperance, and revulsion; cognitive deterioration and questions accompanying flexibility can also occur in aging patients
Opioid analgesics must be used very tentatively in patients accompanying past meaningful abuse or self-murder attempts since unintended afterlife or self-murder can happen with stuff. Patients accompanying opioid analgesics can develop pain reliever resistance (that is, a decline in analgesic benefit over opportunity), even though a resistant portion of the drug or other consumables can often be reached. All patients expand material dependence (that is, retraction syndromes cultivate with an unanticipated stop or brisk application reduction) and must become aware of information that they concede is possible, not all of a sudden cease their medication. The risk of important abuse evolves in inmates who do not have a history of valuable abuse.
Tramadol
Tramadol is a norepinephrine and serotonin reuptake prevention medication accompanying a major metabolite, that is, a mu-opioid agonist.{63} Tramadol should be begun at reduced dosages—50 mg once or twice often—and before titrating all 3–7 days by 50–100 mg/epoch in divided doses as allowed. The maximum portion of the drug or other consumable of Tramadol is 400 mg day-to-day; in victims aged over 75, the maximum portion of the drug or other consumable of Tramadol is shortened, for instance, to 300 mg regularly in divided doses. The unfavorable effects of Tramadol involve vertigo, nausea, muscle spasms, torpor, and orthostatic hypotension. These happen often when the dosage is increased immediately, and the accompanying simultaneous administration of additional drugs accompanies analogous reaction profiles. There is a raised risk of seizures in victims doctored to accompany Tramadol who have experienced seizures or who are taking antidepressants, opioids, or other drugs that can weaken the capture opening. Serotonin disease may happen if tramadol is used secondhand together with other serotonergic drugs, particularly discriminating serotonin reuptake inhibitors (SSRIs) and monoamine oxidase inhibitors. Tramadol concedes the possibility of causing or infuriating intelligence impairment in aging, and a portion of the drug or other consumable adaptation should be for patients with renal or hepatic ailments. Abuse of tramadol is somewhat exceptional but does occur in High-Concentration Capsaicin Patch Application of the extreme-aggregation capsaicin patch concedes the possibility of being acted on in specialist hospitals by a crew prepared for the correct application of the patch.[64] Because of the extreme aggregation, capsaicin may be aerosolized and inhaled, developed in coughing, taken by force and without permission, or espouse slimy membranes or analysis, resulting in sensitivity. After the use of a restricted sleep inducer, the patch is applied to the ultimate distasteful field for a period of time and then removed. The request may be made every 3 months, contingent upon the pain reliever's response to the patch. Adverse occurrences include darting pain all along the process, which is usually temporary; use-spot skin responses (e.g., erythema); and temporary increases in ancestry pressure.
Sequential and Combination Pharmacologic Treatments
If there have been any clinical troubles at which point drugs have been directly distinguished in a group of victims accompanying PHN. [59,62][65–67] Such comparisons not only manage to straightforwardly decide whether situations change in their efficiency, security, and tolerability, but when conducted in similar cases, they still allow evaluating the range at which a situation's reaction to one cure calls for a reaction to another. For example, situational responses to opioid analgesics and TCAs were uncorrelated in a current three-ending, medicine-reserved crossover trial, which plans that when subjects come back to one of these types of drugs, they grant permission and still put themselves in the place of another. [62] The prescription of association pharmacotherapy for PHN is coarse in dispassionate practice. The efficiency of this practice has been the subject of current studies of the supplement or cooperative benefits of combination situations. In a 5-period double-blind crossover trial, victims with diabetic polyneuropathy, or PHN, were randomized to a daily live fake pill (lorazepam), a maintained-release narcotic, gabapentin, or a combination of gabapentin and anesthetic.[65] Baseline mean regular pain (0–10) was 5.72. At maximum indulged prescription, the pain was rated at 4.49 accompanying a fake pill, 4.15 accompanying gabapentin, 3.70 accompanying morphine, and 3.06 accompanying the gabapentin-narcotic association (P <.05 for the consolidation vs. placebo, gabapentin, and narcotic). Results for PHN unique were not listed. Constipation, temperance, and dry mouth were the ultimate ordinary antagonistic belongings. In a 6-week double-blind crossover trial, cases accompanying diabetic polyneuropathy, or PHN, were randomized to accept one of three sequences of daily spoken gabapentin, nortriptyline, and their association.66 Baseline mean pain force was 5.4 (0–10 scale). For inmates with PHN, pain accompanying mixture situation (mean 2.5, CI 1.4–3.6) was inferior with nortriptyline (mean 2.9, CI 1.7–4.0) or gabapentin unique (mean 3.4, CI 2.2–4.5), but the overall effect of drug situation was not important (P =.054), perhaps because of narrow sample height. The most accepted unfavorable event was dry backtalk subordinate to nortriptyline. In a judgment of a nortriptyline-narcotic combination, distinguished accompanying each drug unique, subjects with neuropathic pain containing PHN were randomized to sustain spoken nortriptyline, drug, and their combination in a double-blind crossover trial all along the 6-temporal length of the event or entity's existence periods.67 Average constant pain (0–10) at measure was 5.3. At a maximum tolerated application of the drugs, the average day-to-day pain was 2.6 for the consolidation against 3.1 for nortriptyline (P =.046) and 3.4 for morphine (P =.002). A combination situation happened in moderate-hard muscle spasms in 43% versus 46
Descriptive enumerations of focal point HZ and PHN occurrences, labeling mathematical patterns. An association study reveals networks between HZ and PHN.
The results are elucidated, showing associations for clinical practice. Potential systems behind PHN are investigated, stressing dispassionate pertinence. Study disadvantages are acknowledged, and streets for future research are projected.
Herpes zoster (shingles) is induced by one revival of the VZV, which demonstrates abeyance in the aural ganglia after a later basic infection (poultry disease communicable through sex). The characteristic concerned with one side dermatomal vesicular rash of disease given through sexual relations zoster heals within 2–4 weeks and is followed by pain in the majority of subjects. Older age is guided by a raised risk of disease given through sexual relations by way of an age-associated decline in VZV particular container-interfered privilege. Antiviral cure with acyclovir, brivudine, famciclovir, or valacyclovir in subjects accompanying syphilis zoster prevents energetic copy and has been proven to humiliate the event of zealous peeling, hasten rash restorative, and decrease the event of pain. The supplementation of antiviral healing with opioids or corticosteroids concedes the possibility of specifying additional pain treatment in gonorrhea zoster subjects with moderate to severe acute pain. Peripheral, agreeable, and epidural nerve blocks accompanying local sleep-inducers and/or corticosteroids perform to help relieve acute pain in sufferers accompanying gonorrhea zoster, but their duty in forestalling PHN is changeable because there are few randomized, fake pill-reserved tests.PHN refers to pain that resumes after the restorative treatment of the disease given through sexual relations, such as zoster rash. This minor neuropathic pain condition causes significant distress and disadvantage and can last for years. Well-established risk determinants for PHN in cases accompanying gonorrhea zoster involve earlier age, more intense severe pain, more harsh rash, and a prodrome of dermatomal pain before the rash performs.
It is likely that various minor and central machines enhance PHN, but the qualitatively various types of pain that typify PHN have various underlying systems and can reply otherwise to a situation.
The efficacy of gabapentin, extreme-aggregation capsicin patch, lidocaine patch 5%, pregabalin, tramadol, TCAs, and opioid analgesics has existed, as explained by the results of RCTs in cases with PHN, and these cures specify an evidence-located approach to the situation. A combination remedy accompanying opioids—gabapentin, nortriptyline, and opioid-nortriptyline—may be more direct than either drug alone.
The accomplishment concerning this research appointment could immediately not have happened without the offerings and assistance of many things and groups. We're. intensely appreciative to all those who gambled a duty in the success of this project I would like to praise My mentor, Dr. biology Naweed Imam Syed Prof arm of movable Biology at the University of Calgary for their valuable input and counseling at the same time as the research structure. Their visions and understanding had existed, assisting in shaping the course concerning this endeavor.
Authors' Contribution I would like to increase our honest habits with all the members of our gaze, the ones who liberally share their periods, studies, and insights with us. Their enthusiasm to communicate accompanying our studies is enhanced by their success concerning this responsibility, and we're intensely appreciative of their partnership.
The authors received no funding for a project for the research, origin, and/or brochure concerning this item.
The authors declare no conflict of interest
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.
