AUCTORES
Globalize your Research

case Report | DOI: https://doi.org/10.31579/2690-8794/253
1Radiology Department, Usmanu Danfodiyo University, Sokoto
2Radiology Department, Federal Medical Center, Bida.
3Radiology Department, Gombe State University, Gombe.
4Radiology Department, Usmanu Danfodiyo University Teaching Hospital, Sokoto.
*Corresponding Author: Sule Muhammad Baba, Usmanu Danfodiyo University Sokoto.
Citation: Shamaki AMB, Sule MB, Erinle SA, Aminu UU, Gele IH, (2025), Giant Intravesical Calclus in The Adult Male: A Report of Two Cases, Clinical Medical Reviews and Reports, 7(2); DOI:10.31579/2690-8794/253
Copyright: © 2025, Sule Muhammad Baba. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 February 2025 | Accepted: 27 February 2025 | Published: 06 March 2025
Keywords: giant; calculus; urinary bladder; obstructive
A calculus weighing more than 100gram in weight or larger than 4cm in dimension within the urinary bladder is termed a giant vesical calculus and most often associated with bladder outlet obstruction. Urinary bladder calculi account for about 5% of all cases of urinary tract calculi. Giant urinary bladder calculus are relatively rare and only few cases have been reported in literature and only one case from Africa, with more prevalence among the male gender.
We report two cases of giant urinary bladder calculus in two male adults with obstructive symptoms, they each had abdominal radiography (kidney, ureter and bladder view) that demonstrated oval opacity of calcific density occupying most part of the pelvic cavity; the first case measured about 90mm x 90mm, while the second case measured about 105mm x 105mm in dimension respectively. Both cases were advised to go for further clinical evaluation and assessment by a urologist.
We report two cases of giant bladder calculi incidentally diagnosed following plain abdominal radiography due to its rare occurrence and to review the literature
Giant urinary bladder calculus (GUBC) is relatively rare and presumed to occur from the nidus of an infected material or from a single ureteric calculus with associated progressive layer-wise deposition of calcified matrix most times in a setting of bladder outlet obstruction [1-2].
Giant urinary bladder calculi are those stones weighing more than 100 grams or measured to be larger than 4 cm in largest diameter, with fewer than 30 cases reported in the English literature [1-4]. Most urinary bladder calculi are opaque on plain radiography and composed of triple phosphate, calcium oxalate and calcium carbonate[1-2].
Calculus within the urinary bladder is relatively uncommon and most times accompany lower urinary tract obstruction as a cause, however significant cases may occur without associated bladder outlet obstruction [5-6]. Dietary intake and amount of fluid intake are also attributed to be important factors in the development of bladder calculi [7-8].
Urinary bladder calculus usually present with recurrent urinary tract infections, hematuria, inability to pass urine, azotemia and suprapubic pain or discomfort [7,9-10].
In urinary bladder calculus formation, stasis of urine from causes which can either be benign prostatic hyperplasia, urinary tract infection, urethral stricture, neurogenic bladder, usually lead to the formation of calculus in the urinary bladder [11-12].
Imaging plays a role in the detection of urinary calculus, the calcium composition makes it visible on plain radiography, however other imaging modalities like ultrasonography, computed tomography and cystography are also employed in demonstrating urinary bladder calculus [13].
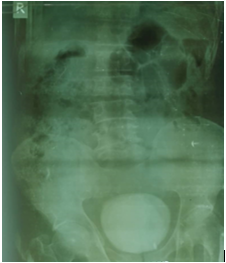
Case 1: this is a fifty-year-old farmer who presented from a peripheral facility for a plain abdominal radiograph (KUB view) on account of recurrent lower urinary tract symptom (LUTS). Some of these are incomplete bladder emptying, irritation along the penile and supra-pubic region with poor and splitted urinary stream. The patient is conscious and oriented, with no sign of palor, cyanosis or dehydration. The KUB demonstrated an oval opacity of calcific density occupying most part of the pelvic cavity; this measured about 90mm x 90mm in dimension (Figures 1 and 2). A complementary abdominal and pelvic ultrasonography demonstrated a curvilinear echogenicity casting marked posterior acoustic shadow with associated bladder wall thickening and moderate hydroureteronephrosis bilaterally. Prostatic enlargement of about 58millilitre was also demonstrated most likely from benign prostatic hyperplasia (BPH). A diagnosis of a giant vesical calculus in a patient with features of BPH and bladder outlet obstruction was made. The patient was advised to go for further clinical evaluation and assessment with possible intervention by an expert urologist.
Figure 1: A KUB; demonstrates a huge, oval opacity of calcific density within the pelvic cavity measuring about 90mm x 90mm in dimension in keeping with a giant intravesical calculus (Left blue arrow).

Figure 2: A KUB demonstrates degenerative changes involving the lumbar spine, iliac and pubic bones with both hip joints. The previously describe oval opacity of calcific density is also demonstrated occupying the pelvic cavity.
Case 2: this is a sixty-five-year-old retired civil servant who presented from a peripheral facility for a plain abdominal radiograph (KUB view) on account of recurrent lower urinary tract symptom (LUTS). Some of these are incomplete bladder emptying, irritation along the penile and supra-pubic region with poor and splitted urinary stream. The patient is conscious and oriented, with no sign of palor, cyanosis or dehydration. The KUB demonstrated an oval opacity of calcific density occupying most part of the pelvic cavity; this measured about 105mm x 105mm in dimension (Figures 1 and 2). A complementary abdominal and pelvic ultrasonography demonstrated a curvilinear echogenicity casting marked posterior acoustic shadow (figure 3) with associated bladder wall thickening and moderate hydroureteronephrosis bilaterally. Prostatic enlargement of about 63millilitre was also demonstrated most likely from benign prostatic hyperplasia (BPH). A diagnosis of a giant vesical calculus in a patient with features of BPH and bladder outlet obstruction was made. The patient was advised to go for further clinical evaluation and assessment with possible intervention by an expert urologist.
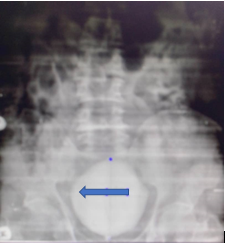
Figure 1: A KUB; demonstrates a huge, oval opacity of calcific density within the pelvic cavity measuring about 105mm x 105mm in dimension in keeping with a giant intravesical calculus.

Figure 2: A KUB demonstrates degenerative changes involving the lumbar spine, iliac and pubic bones with both hip joints. The previously describe oval opacity of calcific density is also demonstrated occupying the pelvic cavity.
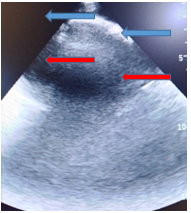
Figure 3: A pelvic sonogram demonstrating a curvilinear echogenicity superiorly (left blue arrow), seen casting marked acoustic shadow posteriorly (left red arrow) within the urinary bladder in keeping with an intravesical calculus.
Giant urinary bladder calculi are those stones weighing more than 100 grams or measured to be larger than 4 cm in largest diameter, with fewer than 30 cases reported in the English literature [1-4].the index cases have confirmed calculi within the urinary bladder and each measure more than 4cm in widest diameter, thereby conforming to these literatures.
Most urinary bladder calculi are opaque on plain radiography and composed of triple phosphate, calcium oxalate and calcium carbonate [1,2]. The cases under review had oval opacity following plain radiography and most likely composed of calcium (reason for being opaque on plain radiographs), thereby conforming to these literatures.
Calculus within the urinary bladder is relatively uncommon and most times accompany lower urinary tract obstruction as a cause, however significant cases may occur without associated bladder outlet obstruction [5,6]. The cases presented also have associated lower urinary tract symptoms with features suspicious of bladder outlet obstruction (BOO), thereby agreeing with these literatures.
Dietary intake and amount of fluid intake are also attributed to be important factors in the development of bladder calculi [7,8]. In this environment, patients are prone to excessive intake of meat, milk and other animal protein, they also have poor intake of fluid, these are indeed factors associated with urinary calculi formation. These cases presented also attested to these dietary and poor fluid intakes, thereby agreeing with these literatures.
Urinary bladder calculus usually presents with recurrent urinary tract infections, hematuria, inability to pass urine, azotemia and suprapubic pain or discomfort [7,9-10]. The cases under review are no exception, they presented with some of these symptoms, thereby conforming to these literatures.
In urinary bladder calculus formation, stasis of urine from causes which can either be benign prostatic hyperplasia, urinary tract infection, urethral stricture, neurogenic bladder, usually lead to the formation of calculus in the urinary bladder [11-12]. Both cases had features of urinary tract infection from laboratory and radiologic evaluation(mobile echoes in urine, bladder wall thickening with increased renal cortical echoes following ultrasonography), features of prostatic enlargement also clinically are ultrasonographically were present. These findings are conforming to that reported in these literatures.
Imaging plays a role in the detection of urinary calculus, the calcium composition makes it visible on plain radiography, however other imaging modalities like ultrasonography, computed tomography and cystography are also employed in demonstrating urinary bladder calculus [13] .the cases under review were also diagnosed following plain radiography and ultrasonography, thereby conforming to this literature.
Basically, giant bladder calculus is treated by open surgical removal called open cystolithotomy. Minimally invasive procedures like cystolitholapaxy cannot be done due to their large size [14,15]. These patients were advised to consult an expert urologist for the most preferred treatment available.
Giant urinary bladder calculi are relatively rare and often accompany bladder outlet obstruction, when suspected basic radiologic examination like plain radiography and ultrasonography do play role in their diagnosis.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

















































