
Research Article | DOI: https://doi.org/10.31579/2693-2156/158
Department of cardiovascular surgery of Mohamed Abderrahmani specialized hospital, 16013, Algiers, Algeria.
*Corresponding Author: Abdelkader Boukhmis, Department of cardiovascular surgery of Mohamed Abderrahmani specialized hospital, 16013, Algiers, Algeria.
Citation: A. Boukhmis, H. Himeur, A. Haddad, A. Moussaoui, N. Medjber, Y. Fellague Chebra, A. Allaoui, B. Djafer, (2026), Gender Disparities in Coronary Artery Bypass Grafting Outcomes: a Single-Centre Prospective Study, J Thoracic Disease and Cardiothoracic Surgery, 7(1); DOI:10.31579/2693-2156/158
Copyright: © 2026, Abdelkader Boukhmis. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 January 2026 | Accepted: 19 January 2026 | Published: 02 February 2026
Keywords:
Objectives: Recent publications highlighted higher operative mortality in women compared to men following isolated coronary artery bypass grafting. Our objective was to evaluate the sex differences of this procedure in our country.
Methods: This prospective, observational, comparative, single-centre study included 260 consecutive patients who underwent isolated coronary artery bypass grafting, of whom 18.84% were women. Women were older than men (61.8 VS 58.7 years, p=0.04), had more arterial hypertension (85.7% VS 62.1%, p=0.001), and more preoperative strokes (8.2% VS 4.3%, p=0.04). All coronary artery bypass grafting procedures were on pump, and bilateral internal thoracic artery grafting was avoided in obese and diabetic women, as well as in patients over 70 years of age. The gender comparison was based on surgical techniques and operative mortality and morbidity.
Results: Although women benefited from the same rate of complete myocardial revascularization (Women: 77.5% vs. Men: 75.8%, p=0.85), they received fewer multiple arterial coronary grafting (Women: 36.7% VS Men: 60.2%, p=0.003) and total arterial coronary grafting (Women: 28.5% VS Men: 48.8%, p=0.01). Operative mortality tended to be higher in women (Women :6.12% VS Men: 2.37%, OR: 2.67, 95% CI: 0.40-14.30, p=0.17), while operative morbidity was similar to that of men: stroke (Women: 0% vs. Men: 2.8%, p=0.59), myocardial infarction (Women: 6.1% vs. Men: 5.7%, p=1) and deep sternal wounds infections (Women: 2.04% VS Men: 0.94, p=0.45).
Conclusion: Algerian women undergoing isolated coronary artery bypass grafting have more co-morbidities, are less likely to benefit from multiple and total arterial grafting and tend to have higher operative mortality rate than men.
ANOVA: analysis of variance test
BITA: bilateral internal thoracic artery.
BMI: body mass index.
CABG: coronary artery bypass grafting.
CAD: coronary artery disease.
CI: confidence interval.
DSWI: deep sternal wound infections.
Euro SCORE II: european System for Cardiac Operative Risk Evaluation II.
ITA: internal thoracic arteries.
LVEF: left ventricular ejection fraction M: men.
MACCE: major cardiac and cerebrovascular events.
MI: myocardial infarction.
OR: odds ratio.
SPSS: statistical Package for the Social Sciences.
W: women
Currently, data enabling appropriate guidance on coronary artery bypass grafting (CABG) in women are limited, and the earliest studies that greatly influenced international guidelines were conducted exclusively in men [1, 2]. Thus, current evidence regarding coronary artery disease (CAD) in women is no more than an extrapolation from that in men.
Recently published studies report on the epidemiological [3], pathological [4, 5], and clinical specificities of ischaemic heart disease in women. American registries [7] and recent meta-analyses [8] highlight the more severe comorbidities of women who are considered for CABG, their low likelihood of access to multiple and total arterial bypass techniques [6], and their higher operative and late morbidity and mortality rates.
In light of these publications, we conducted this study to elucidate gender disparities in CABG outcomes in our country.
This is a prospective, observational, comparative and a single-centre study conducted in a cardiac surgery department in Algiers.
After obtaining approval from the expert committee of the Faculty of Medicine in Algiers, we prospectively collected data on 260 consecutive patients, 18.84% (n=49) of whom were women, who were referred for isolated CABG. Data collection was prospectively performed using patient records.
The gender comparison criteria were: cardiovascular risk factors, preoperative comorbidities, surgical techniques, operative mortality and morbidity: stroke, myocardial infarction (MI), and deep sternal wound infections (DSWI).
All interventions carried out in this study involving human participants were in accordance with the ethical standards of the Faculty of Medicine of Algiers and those of the Helsinki Declaration (1964, amended most recently in 2008) of the World Medical Association. Informed consent for an isolated CABG was obtained from all participants.
We included all consecutive patients aged between 18 and 85 who underwent isolated CABG. Exclusion criteria: combination with another cardiac surgical procedure, particularly valve surgery. Redo CABG or CABG performed as an emergency procedure.
Isolated CABG was performed via median sternotomy with a normothermic cardiopulmonary bypass. Cardioplegic arrest was achieved using cold blood cardioplegia. Bilateral internal thoracic artery (BITA) grafting was avoided in obese and diabetic women, as well as in patients over 70 years of age and those suffering from chronic lung disease. Internal thoracic arteries (ITAs) were harvested in a skeletonised fashion, and proximal anastomoses to the ascending aorta were performed under total aortic cross-clamping.
Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) version 19.0 software (SPSS Inc., Chicago, Illinois). Baseline characteristics were presented as median and standard deviations for continuous variables and count (percent) for categoric variables. The counts and frequencies were compared using the chi-square test, Fisher's exact test, and their odds ratios with a 95% confidence interval. The averages were compared using the analysis of variance test (ANOVA). The p-value is considered statistically significant if it is less than 0.05.
Women (W) were older than men (M) (W: 61.8 +/-10 years VS M: 58.7+/-9.6 years, 95% CI -6.1215-0.0785, p=0.04), with a sex ratio ranging from 1W /10.5M in patients under 45 years of age to 1W /1.1M in those over 75 years of age (Figure 1).
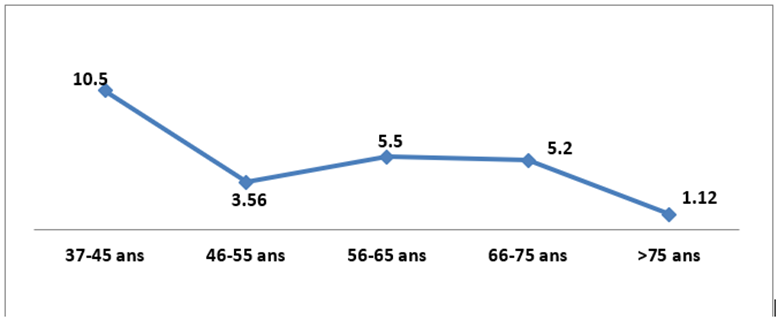
Figure 1: Evolution of the sex ratio according to patient age
The proportion of patients presenting with diabetes mellitus and dyslipidemia was not statistically different between the two genders (Table 1).
| Women | Men | ||
| Âge (year) | 61.8 +/- 10 | 58.7+/-9.6 | 95% CI [6.121-0.078], p= 0.04 |
| Hypertension | 85.7% (42/49) | 62.1% (131/211) | OR : 3.648, 95% CI [1.526-10.096], p=0.001 |
| Hyperlipidemia | 61.2% (30/49) | 56.4% (119/211) | OR : 1.219, 95% CI [0.619-2.449], p=0.63 |
| Obesity (BMI≥30Kg/m²) | 39% (19/49) | 25% (53/211) | OR :1.931, 95% CI [0.943-3.892], p=0.07 |
| Diabètes mellitus | 69.4% (34/49) | 58.3% (123/211) | OR : 1.619, 95% CI [0.801-3.403], p=0.194 |
| Current smoking | 10.2% (5/49) | 59.2% (125/211) | OR : 12.79, 95% CI [4.87-33.57], p< 0> |
Table 1: Sex differences in cardiovascular risk factors.
BMI: Body mass index, CI: confidence interval, OR: Odds ratio, p= p-value.
While women were more frequently affected by high blood pressure (OR: 3.65, 95% CI: 1.53-10.09, p=0.001) and had a strong tendency to be obese (BMI ≥30 kg/m²) (OR: 1.93, 95% CI: 0.94-3.89, p=0.07), the proportion of active smokers was significantly higher among men (Table 1).
Women had a strong tendency to present more atrial fibrillation (OR: 3.29, 95% CI: 0.78-12.69, p=0.053), had more strokes (OR: 3.95, 95% CI: 0.85-14.88, p=0.04), and a lower creatinine clearance than men (p=0.02). Conversely, men had a strong tendency to have more previous
hospitalizations for acute coronary syndrome (OR: 1.8, 95% CI: 0.94-3.45, p=0.081) and had more impaired left ventricular ejection fraction (LVEF˂50%) than women (OR: 2.44, 95% CI: 1.08-5.49; p=0.035) (Table 2).
On the other hand, there were no statistically significant differences between the two sexes in terms of the occurrence of Left main coronary artery diseases (p=0.16) or triple vessel disease (p=0.63) (Table 2) or in the operative mortality risk estimated by the European System for Cardiac Operative Risk Evaluation II (EuroSCORE II): Women: 1.70+/-1.26% VS Men: 1.48/-1.38%, 95% CI: -0.64-0.20, p=0.3. (Table 2).
| Comorbidities | Women | Men | ||
| ACS History | 61.3% (30/49) | 73.9% (156/211) | OR : 0.558, 95% CI [0.278-1.139], p=0.08 | |
| Atrial fibrillation | 10.2 % (5/49) | 3.3 % (7/211) | OR : 3.291, 95% CI [0.786-12.699], p= 0.053 | |
| Extracardiac arteriopathy | 20.4% (10/49) | 23.7% (50/211) | OR : 0.826, 95% CI [0.343-1.84], p= 0.70 | |
| Stroke | 8.16 % (4/49) | 4.26% (9/211) | OR : 3.952, 95% CI [0.854-14.878], p=0.039 | |
| chronic lung disease | 4.08% (2/49) | 5.7% (12/211) | OR : 0.706, 95% CI [0.074-3.339], p=1 | |
| CrCl ml/min | 84.8+/-29.8 | 95.1+/- 29 | 95% CI (1.197-19.403), p=0.02 | |
| LVEF | 57.9 +/-12.7 % | 54.5+/-12.38% | 95% CI (-7.285-0.485), p = 0.086 | |
| LVEF˂50% | 16.3% (8/49) | 32.2% (68/211) | OR : 0.412, 95% CI [0.158-0.953] ; p=0.03 | |
| LMCA diseases | 12.2% (6/49) | 21.8% (46/211) | OR : 0.502, 95% CI [0.164-1.286], p=0.16 | |
| Triple vessel diseases | 59.2% (29/49) | 54.5% (115/211) | OR : 1.209, 95% CI [0.617-2.41], p=0.63 | |
| EuroSCORE II | 1.70+/-1.26 | 1.48+/-1.38 | 95% CI (-0.644-0.204), p= 0.308 | |
Table 2: Sex differences in preoperative comorbidities
ACS: Acute coronary syndrome, CI: confidence interval, CrCl: Creatinine clearance, EuroSCORE II: European System for Cardiac Operative Risk Evaluation II, LMCA: Left main coronary artery diseases, LVEF: Left ventricle ejection fraction, OR: Odds ratio, p= p-value.
Although women benefited from the same rate of complete myocardial revascularization (W: 77.5% VS M: 75.8%, p=0.85), and the same rate of distal coronary anastomoses per patient (W: 2.24+/-0.9 VS M: 2.34+/-0.84, p=0.45) than men, they benefited from fewer multiple -arterial coronary grafting (W: 36.7% VS M: 60.2%, OR: 0.38, 95% CI: 0.19-0.76, p=0.003) and total-arterial bypass grafting (W: 28.5% VS M: 48.8%, OR: 0.42, 95% CI: 0.12-0.86, p=0.01) (Table 3).
| Women | Men | ||
| Number of distal anastomoses/patients | 2.24+/-0.90 | 2.34/-0.84 | 95% CI [0.166-0.366], p = 0.45 |
| Complète Revascularization | 77.5% (38/49) | 75.8% (160/211) | OR : 1.101, 95% CI [0.505-2.567], p= 0.85 |
| MAG | 36.7% (18/49) | 60.2% (127/211) | OR : 0.385, 95% CI [0.19-0.763], p=0.003 |
| TAG | 28.5% (14/49) | 48.8% (103/211) | OR : 0.421, 95% CI [0.197-0.857], p=0.01 |
Table 3: Sex differences in coronary artery bypass grafting techniques.
BMI: Body mass index, CI: confidence interval, MAG: Multiple arterial grafting, OR: Odds ratio, p= p-value. TAG: Total arterial grafting.
Although operative mortality was not statistically different between the two sexes, it tended to be higher in women (W: 6.12% VS M: 2.37%, OR: 2.67, 95% CI: 0.40-14.30, p = 0.17) and seems to be driven by a tendency to develop more postoperative low cardiac output (OR: 2.246, IC à 95% [0.474-8.835], p=0.24) (Table 3).
| Operative mortality and morbidity | Women | Men | |
| Operative mortality | 6.12% (3/49) | 2.37% (5/211) | OR : 2.6739, 95% CI [0.4011 ; 14.309], p=0.17 |
| LCO | 8.16% (4/49) | 3.79% (8/211) | OR : 2.247, 95% CI [0.474 ; 8.835], p=0.24 |
| Stroke | 0% (0/49) | 2.8 % (6/211) | P=0.35 |
| MI | 6.1% (3/49) | 5.7% (12/211) | OR : 1.081, 95% CI [0.188- 4.235], P=1 |
| DSWI | 2.04% (1/49) | 0.94% (2/211) | OR : 2.2521, 95% CI [0.037-44.198], p=0.45 |
Table 4: Gender disparities in mortality and morbidity associated with isolated CABG
CI: confidence interval, DSWI: Deep sternal wound infection, LCO: Low Cardiac output, MI: Myocardial infarction, OR: Odds ratio, p= p-value
There was parity between the sexes concerning stroke (W: 0% VS M: 2.8%, p=0.59), MI (W: 6.1% VS M: 5.7%, OR: 1.08, 95% CI: 0.19-4.23, p=1) and DSWI rate (W: 2.04% VS M: 0.94%, OR: 2.2521, 95% CI: 0.037-44.198, p=0.45).
The main conclusions of this prospective study are as follows:
Underestimated for a long time, cardiovascular disease is currently the number one killer of women in the United States, where it accounts for a third of all female deaths, surpassing the mortality rate caused by all female cancers combined. Between 1984 and 2012, more women died from cardiovascular disease than men [3].
In addition to the classic cardiovascular risk factors common to both sexes, women are also subject to specific cardiovascular risk factors, such as: preterm delivery, gestational hypertension, gestational diabetes, autoimmune diseases, breast cancer treatments (radiotherapy and chemotherapy), and depression [4, 5]. Furthermore, the influence of various risk factors differs between the two sexes. The harmful impact of smoking is more pronounced in women than in men. Moreover, menopause has a significant effect on women, as there is a higher incidence of plaque rupture in older women [9]. The multiplicity of these cardiovascular risk factors, to which women are exposed from a young age, gives their coronary artery disease a particular anatomical and pathological feature. Indeed, coronary lesions in young women tend to be diffuse and non-obstructive. Smilowitz et al [10] has observed that myocardial infarctions secondary to non-obstructive coronary lesions are more common in women. With age, coronary lesions in women become increasingly obstructive, gradually resembling those in men. Women often present with coronary microcirculation dysfunction, endothelial dysfunction, limited coronary flow reserves, spontaneous coronary artery dissections, more frequent intramyocardial coronary arteries, and stress-induced cardiomyopathies (Takotsubo) [4, 5, 9].
Several studies have highlighted the particularity of coronary artery disease symptoms in women, as well as their lower chances of receiving the same standard of treatment as men [11-13]. In fact, women become symptomatic on average 10 years later than men, and their symptoms are often atypical, sometimes leading to misdiagnosis. They suffer from more comorbidities and develop more silent myocardial infarctions and sudden deaths. They often present with more invalidating symptoms despite angiographically insignificant lesions, indicating involvement of their microcirculation. In addition, they are less likely than men to receive optimal medical treatment. These diagnostic delays and disparities in preoperative care explain the poorer clinical profile of women candidates for CABG and inevitably lead to different surgical outcomes compared to men.
A recent study of the American registry [14], including 2.5 million patients, 28% of whom were women, noted that after isolated CABG, women were associated with a persistent increase, over a 12-year period, in the adjusted risk of all-cause mortality (OR: 1.43), stroke (OR: 1.34) and thoracic complications (OR: 1.28). This finding was also mentioned in a recent meta-analysis [8], which showed that women were associated with a higher risk of operative and late mortality as well as post-operative MI and stroke than men. Furthermore, a systematic review of four randomised studies (ART, CORONARY, GOPCABE, PREVENT IV) [15] noted that although 5-year mortality was equal between the two sexes, the rate of major cardiac and cerebrovascular events (MACCE) was higher in women, driven by a higher rate of MI at 30 days and, consequently, a higher rate of repeat revascularization. It has also been mentioned that the difference between the two sexes in terms of in-hospital mortality and MACCE five years after an isolated CABG is inversely correlated with age. These differences are greatest in young subjects and tend to disappear after the age of 75 [15, 16]. This levelling out with age of gender differences in CABG morbidity and mortality can be explained by the fact that coronary lesions in women become more obstructive with age, thus resembling those in men more closely; furthermore, the spasticity of coronary arteries and arterial grafts in women decreases with age, thereby reducing the incidence of MI; and finally, comorbidities in men increase with age, thus matching those in women.
In our study, women were less likely to receive multiple-arterial or total-arterial coronary bypass surgery. There are two explanations for that: (a) on the one hand, the combination of diabetes and obesity, which was more common among our female patients, would have exposed them to a much higher risk than men of developing DSWI after BITA grafting [17], (b) on the other hand, in our cohort, the proportion of women over the age of 70 is higher than that of men, and after this age, it has been established that BITA grafting loses its long-term survival benefit compared to the single internal thoracic artery grafting [18]. This finding was recently noted in the Society of Thoracic Surgeons database, which included more than 1.2 million patients who had undergone CABG between 2011 and 2019, confirming that women were significantly less likely to receive complete revascularization, a left ITA-left anterior descending artery grafting, a radial artery as a second graft, or BITA grafting [19].
This inequality in access to optimal CABG surgical techniques is particularly disadvantageous for women, as a recent observational study [20] and a meta-analysis of six randomised studies [21] have clearly demonstrated that the very long-term survival of women is improved, as much as that of men, by BITA grafting, by multiple-arterial bypass grafting, and by complete revascularization.
Furthermore, several authors have reported on the technical complexity of CABG in women. It has been established that the diameter of the major epicardial coronary arteries is smaller in women, even after adjusting for body surface and for left ventricular mass [22]. This may explain the higher proportion of incomplete revascularization in women. In addition, it has been shown that the diameters and flow rates of women's radial arteries are also smaller than those of men, even after adjusting for body mass index [23]. This may explain why it is more difficult to use arterial grafts in women, particularly when performing sequential anastomoses and composite arterial grafts. Furthermore, it has also been shown that arterial grafts from women are more spasmodic and more reactive to vasoconstrictors (ITAs-serotonin and radial arteries-noradrenaline) than those from men [24, 25]. This increased spasmodicity contributes to postoperative spasms in these arterial grafts, which can cause postoperative ischemia or even myocardial infarction, more frequently observed in women.
Based on these studies, the poorer outcomes of isolated CABG in women compared to men can be attributed to:
Limitations of this study are (a) its single-centre nature and (b) its small sample size. A multicentric study conducted over a longer period and involving a larger cohort would yield more statistically robust results.
Algerian women undergoing isolated coronary artery bypass grafting are older, have more comorbidities, have less likelihood of benefiting from multiple or total-arterial bypass grafting, and tend to have higher operative mortality than men.
Disclosure of Funding:
This research did not receive any specific funding from public, commercial or non-profit funding organisations.
Disclosure of any Conflict of interest: None to declare.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
