AUCTORES
Globalize your Research

Review Article | DOI: https://doi.org/10.31579/2639-4162/246
1 Physical Therapist NDT teacher IBITA, Course Leader and teacher on the Dutch Institute for Allied Health Sciences. Nursing Home “Waelwick” in Ewijk the Netherlands.
2 MSc BSc RMN Lecturer in Mental Health Nursing with Dementia Specialty. University of Cumbria, Bowerham Road, Lancaster, LA1 3JD England
*Corresponding Author: Jan van de Rakt, Physical Therapist NDT teacher IBITA, Course Leader and teacher on the Dutch Institute for Allied Health Sciences. Nursing Home “Waelwick” in Ewijk the Netherlands.
Citation: Jan van de Rakt, Steve McCarthy-Grunwald (2025), Balance Training Parkinson, J. General Medicine and Clinical Practice, 8(3); DOI:10.31579/2639-4162/246
Copyright: © 2025, Jan van de Rakt. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 December 2024 | Accepted: 31 January 2025 | Published: 17 March 2025
Keywords: rigidity; parkinson; balance and selectivity
Introduction
The disease Parkinson give all in the beginning problems with walking and especially with the balance. The treatment ideas improve, this is great and is a great achievement, because now have people the feeling be active to “stopped” this disease and indeed, it will slow down the great number of symptoms that makes the quality of life very difficult.
Design of this article: The purpose of the design was to search for the reason, why this aspect- balance- was so fragile and so fast affected. Then is the search for the functioning of the damaged brain the first” stop”, because there will be the answer, why people with this disease are using “cues” to get the influence of that damaged brain under control. Cues are capable to transform a freezing moment in movements- possibilities. That difference must be done in the brain and that means that are different ways to create a movement. Result: This fact that there are more possibilities to get a movement done, means that there is through this disease a problem to choose immediately the optimal way. This -not capable- to choose the optimal way, must have a reason and one of them is that the brain must choose for an pathological tone (rigidity) to master the gravity.
Conclusion: Looking at the way people with the disease of Parkinson move and search for cues to get an better control and get the force of gravity under control, let us believe that this gravity force, forces people to use lower systems with an pathological tone and muscle pattern. This conclusion, direct us, that this gravity force asked for too much tone. That asked for measurement and treatments in which that tone increase isn’t necessary. Soo that the selectivity can be trained on his highest level.
Balance is for all elderly an problem that will grow, when people are getting older and have more problems with free movements, but the adaptation is often very impressive. An lot of elderly have an balance that is still perfect but is an different kind of balance as that of an younger adults. More is needed to hold that level secure and this adaptation must be understood!
Let first look at the balance – counter system and see that the base is the axis “feet” -(feeling) and the “feet”-reaction, the reaction time between the “passive” reaction on an impact and the “active “correction is less than 300 m/s and according their calculations is that within the necessary time to prevent an fall [1]. Further was it clear that other important systems to control the balance has not the direct possibility to react so fast as this axis. That makes this axis the base on the immediately reaction on something that is so abrupt that no preparation is possible and that is the balance system where we are looking at. Figure 1.
On the left side the time that the information is passed through that place and under the onset of the displacement. Here we see that it starts in the feet and go to the head and that this is answered with an active reaction all away back, our base system.
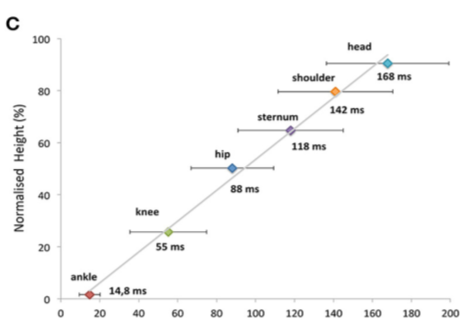
Figure 1. Onset of Segment Displacement. [1]
This base system can thus work optimal when the way to the brain and back is optimal, that means that the feeling system feel adequate and give the right information of what is happen to the brain and that the brain is calculated perfect and give the right output back. This reaction is known for the three basic balance reactions;
Backward fall: asked for the feeling under the feet and the reaction of the feet- dorsal flexion- and flexion in the hips/trunk. Small disturbances will need often only an feet reaction by younger people but by elderly will very soon the flexion of the hip/trunk be necessary to counter. Then we see that the reaction in the feet and trunk are almost on the same time, thus an ankle strategy and hip/trunk strategy are needed to brace the fall movement to do what …--- To get time to bring the whole body weight on one leg and make the other free for stepping away or better to the back. And why is this trunk /hip flexion so important, not only to bring more body to the front but also to initiated the movement of the free leg to the back to make an step-strategy optimal possible.
Forward fall: asked for the feeling under the feet and the reaction of the feet- plantar flexion- and extension in the hips/trunk. Now the back side (back- diagonals [2]) are the dominant muscle pattern group to controlled this movement from feet all away till the neck. This lift on the feet with the extension in hip and trunk is necessary to get time to…shift the weight total to one foot and make the other free for the step- strategy. The extension in trunk /hip will propel the free leg to the front. By elderly will the necessity for the whole reaction be more needed as by young people. That means that feet and trunk are reacting almost on the same time.
Sideway fall: asked for the feeling under the feet and the reaction of the hip/trunk latero- flexion and lift of the trochanter over the lateral side of the foot and later in the feet controlled in-and eversion [3,4,5,6]. This is different with the back- and forward fall, where the feet and trunk/hips react on the same time, by sideway this must be start with an movement in the hip/trunk and so far that the trochanter is over the lateral part of the foot, than the reaction of the foot will go on. See we on the forward fall the action on the backside (back diagonals), by the backward fall will the front diagonals be the most active but by the sideway fall must there be an cooperation between all diagonals and also prominent on the hip-keypoint. Because the elongation and the hip movement make it possible that the free leg can cross and then this leg bear the weight and the other makes an step strategy. The elongation gives the free leg the possibility to make adduction -cross- and an shortening will give the free leg abduction.
By elderly is thus adaptation going on, during years and mostly is that the trunk/hip is used to control their attitude and an better brace of the disturbances of an fall and create more time for;
One of the most done adaptations by elderly is the counter action on the change of the spine attitude.
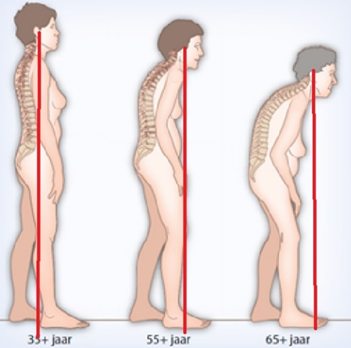
Figure 2
Figure 2: Spine changing and place the trunk an total different position and that asked for an balance adaptation. [7,8] We see that in figure 2, when we follow the red line that start in the ear and goes to the feet and will fall in the heel of the for-standing foot. But when the thoracic spine “collapse” we see that this line goes more to the front of the foot. The consequences of this attitude alternation is that the foot must be faster to the ground and that means that the heel strike will be alter and even disappear. No heel strike will also give an lesser activation of the great hip-extensor and also no movement over the hip when walking.
The foot must faster to the ground to counter the “forward fall” movement and this fall movement asked also for an concentric activity of all back/neck muscles.
It looks like an eccentric action but often starting in the neck is an concentric activity necessary to control this “fall’ movement. The neck extension will have an influence on the stretch on the muscles on the front and indirect on ability to speak, eat and swallow [9].
Investigation about the muscle power of the feet muscles by young people and elderly give an picture that the dorsal flexor are fast losing power and the reason is that too much plantar flexion is necessary, but also they muscle loose power [8]
| Power difference | Healthy young people | Healthy elderly |
| Right dorsal flexor | 11.7 | 8.2 |
| Left dorsal flexor | 11.6 | 8.6 |
| Right plantar flexor | 19.2 | 11.3 |
| Left plantar flexor | 21.7 | 12.2 |
Table 1: Still the adaptation goes on and elderly make automatic changes, hold control over their balance, one of the most use is: 1. Simple- 2. less risks- and 3. slower movements. But an trunk, that has this trunk-attitude, will give by an forward fall more effort to get the free leg to the front because through the trunk position will the free leg go to the back. That has thus consequences when people stumble [10], still according Prof.Robinovitc [11,12] and co, is this not the most common reason that elderly in long car facilities fall.
Stumble
The problem that must solved, is that the leg that hook, get enough time to get to the front to catch the “fall – movement” at the right moment.
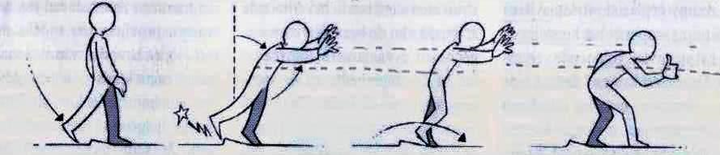
Figure 3
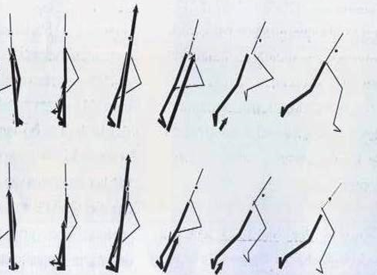
Figure 3 and 4: The stumble activity with one leg behind the other. This asked for an activity of the whole body to brace the fall movement and bring thus the trunk back and create time that the free leg (stumble leg) can passed and place in the front an prevent a fall. Figure 4 let see on the upper row the reaction of young people and the lower of elderly.
In the upper row( young) the diffrences are visble from the third figure from the left, and then clear in the fourth figure. By young poeople the arrow (vector) stay in front of the hip joint and that isn’t the case by the low row (elderly) there is the hip passed this point.
That means;
In this investigation was also an search of the activity of the muscle, when and how much; ( the black line are the young one, the gray line the elderly)

Figure 5
Figure 5: The differences are clear, the amount of muscle power and the moment of action. Still we see one slight difference by the start in the moment that the muscle semitendinosus is active. This could be an sign that here is an medial hamstrings/adductor action necessary and that could be an sign that an pathological neurological synergy is active.
Eyes
The approach to asked more from the other vestibular systems is possible but be aware that this is slower system and never at time to prevent the fall, but of course the contribution to calibrate the system is essential. So also, the activity of the eyes, elderly look often more to the ground and not in the distance to “search” for danger. This is often not good understood and many elderly will be advised to look straight forward but the reason is that these eyes are necessary to create an better control over the system. The feeling of the feet is lesser than is eye control essential. An investigation that place elderly on treadmill above the ground (0.6 metres) [13], let see, how necessary this adaptation is to control walking on it with obstacles and the differences between young and old people and thus also the amount of errors. And that was confirmed by another investigation that found that elderly need more of their brain capacity to walk as young people. An sign that walking asked more than normal and an reason is to control all the adaptations and the balance.
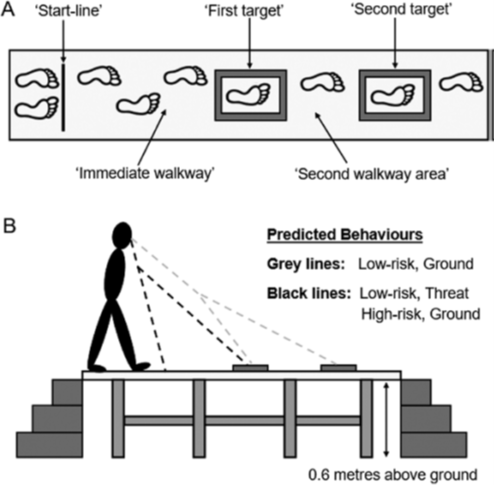
Figure 6: Walking on an treadmill on 0,6 metres height let see that elderly need their eyes to control the area for their feet and that has the consequence that the obstacle is seen too late and that elderly will thus make more errors and stand up the obstacles. But this is an reality and therapist must be certain that this eye control isn’t needed, otherwise we destroy this adaptation!
Capacity
Capacity of the brain is often be pointed as the problem why people with an brain disease fall more and especially people with the disease dementia, but this isn’t clearly a reason but is an factor that has influence on their performance. The amount of activity in the prefrontal part of the brain is by elderly much higher to control the tasks that they must do in comparison with young people ( figure 7) [14] But on the other hand is know that elderly complaint over the balance and walking abilities almost 5-10 years before the diagnosis dementia is determinate and why this is, is still today an item for research but elements could pointed on an pathological neurological tone increase[15,16,17].

Figure 7: An study in which young people were comparison with elderly in three different walking conditions. Usual walking, dual-task walking and walking with obstacles. In this study was measure the blood circulation increase in the prefrontal part of the brain and see the differences because that start by normal - usual- walking and stay high through the other tasks. That means that elderly need more brain capacity to do the same and that is an sign of that adaptation on all levels.
Summary of the introduction:
Elderly must adapt their balance capacity and this process is often years going on, before any therapist has done an investigation what the reason could be that this person fall more than “normal”. The greatest failure is than no individual assessment but an program as “Fall-prevention” because that will never find the missing link, only the determination that this person cannot follow the program.
Adaptation.
This adaptation is normal but by people with an neurological disease are sometimes systems changes that could have fast consequences. Par example the last investigation by an suddenly change as an stroke show that people with an minor damage could still have more problems with their balance, even after an T.I.A.- (Trans Ischemic Attack) was mentioned. Further we know that by stroke the difference between the two sides is great and will lead to an greater fall-danger[18,19] Stroke is an example that adaptation isn’t possible but by other neurological diseases will this play an very important role and therapist must see and recognized that adaptation and what this will have for consequences for an possible treatment to hold the balance and walking capacity on an higher level for an longer time. By an disease as Parkinson we know that the disease will make people dependent from other ways though the brain to hold the balance and walking ability on the highest possible level. This variation of cues on all kinds of input levels to help the damaged brain to find an solution is famous but this asked for an extra stimulus from the outside. There are people that can give their self that cue/ stimulus but still is asked very much of the system and isn´t always perfect.[20] Still many investigations give an positive picture about the training of the Tai Chi approach [21,22] and big movements [23] let see what there possible on treatment area and that is an approach where with an high intensity movement were made and with many rehearsals, where the control on the attitude is great and this give often an good results for an long time but still there are in the progression of this diseases moments that this is going lesser and the influence of the training is also fewer. Here must not end our treatment, but must start the search why the problems by people with Parkinson increase and why this treatment has not the expected results.
What is changed and what is now the next step to try to get the level on his optimum!
Problems as; - Less arm swing, -Walking with more kyphosis, -Freezing, -Stiffness, -Rigidity.
Less arm swing
So characteristic by this disease but we see this also by people that suffer from the disease dementia and always is there an relation with less balance and walking ability.

Photo 1, 2 and 3 are people from almost same age but the gentleman on photo 1 is diagnosed with the disease dementia, Photo 2 disease Parkinson and photo3 is an healthy woman.
Photo 1 give a picture from an man that is walking and there must by an certain speed be an swing of the arms contradictory on the leg movement, but that speed is very slow and thus should there must be an relaxation of the arms. That relaxation is only visible in photo 3. Regrettable, only visible, because this relaxation isn’t measured. Measurement of the resistance of an arm movement in stand or when people are walking will give us the answer of this tone is high, higher than it should be.
| Measurement | Photo 1 | Photo 2 | Photo 3 |
| Anteflexion movement shoulder | Mas-P = 2 | Mas-P = 2 | Mas-P= 0 |
| Retroflexion movement shoulder | Mas-P = 1-2 | Mas-P = 1-2 | Mas-P= 0 |
| Flexion Elbow movement | Mas-P= 2 | Mas-P = 2-3 | Mas-P= 0 |
| Extension elbow movement | Mas-P = 1-2 | Mas-P = 2 | Mas-P= 0 |
Table 2: Measurement tone photo 1,2,3 [24,25,26,27,28,29.30.31]
In this test the movement that we make was measure and thus the opposite muscle. Both gentlemen had an higher tone in the agonist but also in the antagonist [33.] The Mas-P technique is an measurement of paratonia, an neurological pathological tone, that we see by dementia. In this test was the use of the Mas-P the best test-method to do, when people are busy with walking or balance/stand (this last two were reliable) and when the tone resistance wasn’t feel, we use than the Tardieu technique to increase the movement speed [32]. Remarkable, the decrease of the tone and almost normal when this person sit down, certainly after an while. Thus, the conclusion of this measurement is that the two gentlemen need an pathological tone-increase in the upper trunk/arm to control the walking and the balance activity. This measurement reveal that the two persons use in the upper trunk an pathological tone to increase the control.
Photo 1. Walking with the face in one grimace and no deviation of the head. The head stand firm with an stiffness cervical[34]. There is therefore no possibility to look around only straight forward. The upper trunk stand in slight flexion but the shoulder and especially the elbow stand in an upper trunk backward [35], an sign that the tension of the muscles on the backside
is high. And the arm stand almost equal and thus isn’t visible what leg is swing and which is in the stand phase.
Photo 2. A balance training- go so far as possible to the edge of your possibilities to the back. That asked thus for an dorsal flexion of the feet and an flexion of the hip/trunk and an movement of the arms to the front, but…. We see that no fore-feet are of the ground, that the flexion isn’t optimal and that the arms stay behind. This picture let us see that this situation asked for an tension increase of the upper trunk to hold control over the lower trunk and backward movement.
Photo 3 let us see how we go to the back with an normal reaction and see how far she goes and how “low” the tone stay.
This less swing movement is thus because people need to use an higher tension in the upper trunk to make this part stable and give the lower trunk the opportunity to move. But why they use an tone that is pathological and asked thus for much more investigation, but the necessity is certainly still there, because with medication this abnormal tone decrease is often gone during some time.

Photo 4 Photo 5
See difference between the tension in the upper trunk and the relaxation of the arms when this gentleman walks through the corridor, first without his medicines and on photo 5 with his medicines. The difference in the flexion in the upper trunk -left with two arms along the body on the same place and the flexion in the elbow. And look at photo 5, now the flexion in the upper trunk is lesser and also in the elbow.
The medicines [36] will help the damaged brain to get the normal control over the whole senso -motoric system and restore thus the normal selectivity and dexterity and … an normal tone. No resistance was there when we move the arm with speed. But that resistance was present when this he was off medications. That means that the damaged brain must work with the resources that it has and when this walking and control balance than is the best option to let the legs to do the work and hold the rest as stable as possible.
This must it be done with less selectivity /dexterity, because he must do it with an system lower in the brain and that systems use;
1.Pathological synergy; - stereotype movement pattern with little possibility to change, with little freedom-degrees. 2. Second elements is that this pathological synergy uses an pathological tone that will resist normal speed movement because movement must now be done with an slower speed. 3. Thus, the walking and balance must be change in speed, smaller steps and all in the area of good balance and through the stable upper trunk, is this problem solve within the borders of what the damaged brain can.
Thus, increase tension -tone- and thus among other things, more flexion in the elbow is an sign that the stabilization of the upper trunk is necessary, to hold the walking and balance performance intact.

Photo 6: The freezing [38,39,40] of gait by people with the disease of Parkinson is such an strange moment that people are even self so surprised that this is happen. Many have “solutions’ to get out this freezing state and starting with walking but this asked always for an “cue’. Prof. L. Cools [41,42] invest in the last part of the past century, the way people with this disease use to get out this freezing and he say an great scale of ways. But everyone must do, some extra things to overcome this problem or needs help from others to get through this freezing state. Cools call this that the brain isn’t capable to change routes because through the damage this flexibility/ dexterity isn’t possible and must the damaged brain search for an stimulus – an cue- of all kind that give an reaction in the brain that make the person possible to use another way in the brain to accelerate the system. This has also discovered A. Nouws al in the beginning of this disease. [43]
What happen, when people cannot start with an action as walking and freeze? The program to start walking isn’t found and now search the brain for another and the easiest one is an lower system in the brain but…. that will use stereotype movement through pathological synergy with often an higher tone, this is the stiffness that many people feel and that is the “barrier” that this people feel. Measurement of this moment of the tone is not described, as far as we know, but our experience by cases in which the freezing occurs and an measurement was possible, was the tone in the elbow (direction extension first and after that flexion) always higher than Mas-P = 1. At the moment that people had found an different way to counter the freezing was the tone always almost immediately lower but often still was there resistance against an movement with more speed as the Asworth-scale, more according the Tardieu scale. Meaning that the “cue” has an direct influence on the tone through the different “route” in the brain and this route has more selectivity!
Photo 6 let us see the moment that this person stands fixed and the attitude is; Head light flexion, looking at the floor
A.Slight flexion upper trunk, with an upper trunk backward also qua tension because see the shoulder position and the flexion in the elbows. B. The legs stand in hip/ knee in flexion but the legs stand in the mid between endorotation and exorotation and also adduction/abduction, the influence of the pathological synergy is here not direct visible. C. The feet stand in plantar flexion and the weight stand on both feet and that means that it is impossible to lift an leg. (Influence of the synergy!)
Thus no weight shift [11]!
Why there isn’t no or an incorrect weight shift?
The start use an system in the brain that is based on synergy’s and an higher tone and that isn’t selective enough to initiate walking and shift the weight to one side with balance. Now we see the attempt with the upper trunk to the front, almost an falling movement but no shift and thus end this in an fall on the knee or in an state that no movement is possible. The cue will interfere with the system and often take another more selective one and the walking occur and the pathological tone is immediately lower and sometimes gone. But Parkinson disease is an degenerative disease, this this will occur again and the cue will be at the end not work anymore. Even the last cue- the exteroceptive / proprioceptive cues give not the reaction and that means that the damaged brain cannot change the route in the brain anymore.

Photo 7 and Picture 1: Give an image of the dominancy of the pathological synergy with the high tone.
Before the walking can start was an push on the shoulder (Picture 1) necessary, an push in which she was place on her heels and then she was capable to shift the weight and walk but the distance was restricted through the dominancy of the synergy and the tone that increased.
The possibility to switch to another route wasn’t possible anymore. This will happen by everyone but how we can postpone this decline!
Starting with walking with assistance was almost impossible, through the impossibility to shift the weight to one leg and free the other. But when she stands and there was an pressure on her shoulders down in the direction of the heel than was she capable to shift and start walking but still there was an clear influence of the pathological synergy’s and the pathological high tone. This will be go on and will at the end place this people in an attitude with an lot of tone. [44,45] This high tone makes thus selective movements difficult and at the end they dominate. We are aware that this isn’t complete to avoid but we must invest what we can do to control that high tone [46]. The reason that the tone must increase is that the gravity asked for more power and that this demand asked that the brain use other routes to control this. At the moment that we can decrease the influence of the gravity; we see that this selectivity returns and there are examples that by neurological degenerative diseases this occur at moment that nobody taught that this was possible. [47,48] Thus an pull test [49] that is so positive that there seems like there is no reaction, is still an indication to search for an tone decrease treatment and the best way is to decrease the influence of the gravity. The route in the brain on an lower level that use stereotype movements with an high tone must be use to counter the gravity, at the moment that this influence is lesser the reaction could be an route in the brain on an higher level and with more selectivity and often also more cognition. Casus repost about measurement of the Duncan reach test before and after an treatment in the swimming pool give significant improvement, both are taken on land, one for the treatment and the other after the treatment in the pool but done on land on the same spot. [49,50]

Photo 8: The execution of the “Pull-Test “. An test in which the therapist pull at the height of the shoulders to the back and observe the reaction. This person goes as an statue to the back. People that see this think that there isn’t awareness present but that isn’t the case. Look at the feet and we see that right fore foot is up to brace the movement but the left foot shows no reaction of maybe even the opposite, clawing. The arms go somewhat to the front but in the trunk/hip isn’t an track of flexion, necessary to brace the movement and get time for an weight shift and thus an step strategy to place the foot to the back. Here the dominancy of the lower route is present and important is that people measure the tone!
At the moment, that the tone increase and people must use the pathological synergy’s and cannot switch to another route through an cue, than is it important to create an training environment that is an cue and decrease the gravity and thus the necessity of that high tone. To train this from the beginning of the disease will give that this route is more use and better functioning in other situations.
Training in water as an example to lower the gravit !
The literature [52,53] is quite different, from look out and careful, all away till an positive effect on balance etc. in comparison with exercise on land. This difference has to do with the experience of people with Parkinson, when they enter the pool and experience the loss of gravity and growing effect of the upthrust and that asked for an change of an strategy and here is by people with Parkinson the problem. Using the gravity and an cue to move on land isn’t the solution in water where at the moment that the water level increase over thoracic 11 another balance reaction is required than on land. Thus knowing this, is it important to coach people that they are going in the pool and take time to experiences that and learn to deal with it. At the moment that people with Parkinson experiences, that the control isn’t there, is also the moment that this can be the best treatment that this person can have. This because, he use in water his land- route against the gravity and the cue that the water give through upthrust, can he then not translate in an higher route with more selectivity. Often people start to deep, thus above Thoracic 11 and then play the head an important role to control the balance. Goes the head to the front ( looking: “ where are my feet?”) that will the feet go up behind him and he will experience that his legs are leave the bottom and an head extension is necessary to get them back. Go the head in extension too far than go the feet in the front up and must the head movement this correct. Just this group fixated often the cervical spine [34] and the reaction isn’t possible with all dangers that than occur. Fixation of the whole upper trunk give the reaction in shoulder and flexion in the elbows.

Photo 9 Photo 10
Photo 9 and 10: The difference in movement execution, speed and selectivity between this two photos is great, also the pleasure is so different and of course the effort that is made. The heartbeat will be clearly increase and thus also the blood circulation in the brain and that is necessary to stimulate the brain and keep this organ in the best shape.
Training, also in water, asked for rules that must be follow to get the best results of the treatment. Also, by an neurological degenerative disease is it important to hold the rules in the back of the head because training will slow down this disease but will never cure it. Therefore, it is so important to measure the tone and register the pathological synergies, because that will often the threshold for this person to participate with others on an training on land and also the moment that the cues don’t give the effects as before. This moment must be and can be avoid through an training in the water to hold the selectivity as long as possible on an good level but that asked for an regular training in the water with clear training scheme that train all aspects to slow down this disease. Training without measurement is no training, but that measurement must control the treatment. And there are two elements that are important for people with Parkinson to measure and that is the aerobe activity [54] because this has an effect on the blood-circulation of the brain and anaerobe activities and that means that tone but also balance must be measure and then especially what the performance are as one leg standing [55,56.]. Training rules [60,61] together with learning rules [57,58,59] are important to get the best performance and also the best results but people with neurological diseases have the problem that the tone can increase and then is movement restricted or as by balance training even impossible, therefore must the tone down and that can only when the reason – gravity- is decreasing. Strengthening of muscle pattern is only possible when there is an movement against resistance with rehearsal that will give muscle fatigue and that with an certain frequency to stimulated this muscle pattern to increase the coordination [62] and the power of the muscle pattern. This treatment to increase the coordination will be asked for task specific resistance training that are senso-motoric almost equal with the task that we want to train and when possible, with an higher energy cost, because now will this transform in an better muscle pattern system or slow down the decline. Thus, must the environment water be able to give us the possibility to treat on this two (aerobe and anaerobe level) and with the right intensity and also be able to give room to variation or/and other therapy forms that are invest and give an positive result. The answer is so simple, water will be more than able as on land [64] because through the tone lowering. We know that the translation to movement quality on land is present, when there is an good frequency of therapy in the water. Some elements in therapy, that are invest by people with Parkinson often in the beginning phase are Tai Chi [21,22], Big movements [23], boxing and dancing [65,66], let see that there are opportunities to slower down the process by training in that way. Therefore, it is strange that training in water isn’t mentioned from the beginning because Tai Chi is transformed in Ai Chi and the big movement, boxing and dancing are perfect possible in that environment and will contribute in an better training result with less risks.
No balance training on land can ever go so far that the balance is gone and that the reaction isn’t right and an fall occur. This border will on land always an important item that isn’t present in water. The fall in water will be brace through the water and therefore slower than on land but still there is an reaction possible and an failure will not lead to an trauma. Other element is the task specific training, that is pointing on balance training and the muscle pattern are so trained that they are optimal qua coordination and strength (or better power, strength × speed). This asked for an training program that will deliver an muscle fatigue in the task and that task is especially the bracing of the fall movement so that an weight shift and step-strategy is possible. This training must be implicit, the task must be had direct or indirect an connection with the task. Verbal explanation has no value in this training form, but the possibilities are so big. Give some an plank under one foot and ask him to walk with this under his foot to the other side of the pool, what will happen:
Picture 2 Picture 3
Picture 2 and 3: The focus lies on the plank in two or one hand or under one foot. This changes the focus from standing on one leg to control the plank par example under my foot and get him to the front on the floor. That means weight shift and balance but the focus is on the plank and certainly standing on one foot for some tone.
Picture 2 and 3 are only examples of an exercise with the focus on something different as the item where the exercise is intended for. And this exercise is nice, but will the reaction be, an increase of the coordination and the increase of the power of muscle pattern or the aerobe improvement? Therefore, must this training lead to an stimulus that improve and that asked rehearsal which is so heavy that this is an stimulus for the system and that asked for an good frequency, otherwise will this reaction not occur. But don’t forget that this is an degenerative disease and one of the elements that will show that there is an lower level reached, is the increase of the pathological tone and that is an signal that the training must be adapt and that can be in the water to search for more time and depth to have more influence on the tone. And adapt the training program because an exercise that isn’t at the level of the person will have an negative effect on the performance but also on the motivation.
Training of people with the disease of Parkinson is necessary from the beginning of this disease but asked also for an structure in that training. That asked for an training schema and measurement to control that training scheme and an important item in that scheme is the height of the pathological tone. That tone increase, often called stiffness/rigidity, makes movement very difficult and stereotype and destroyed the selectivity/ dexterity that still is present in the brain but is oppressed through the influence of gravity. This stiffness will increase through this brain disease and therefore is it very important that there the focus on is and that by using the environment water and an good training and learning program where there is an training and an problem solving action possible and that will hold the brain in an optimal condition. But be honest what an person can handle and let the training be adapt on the possibilities. Training in water is even possible in the last phase of the disease [67].
Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.





























































