
Research article | DOI: https://doi.org/10.31579/jcpmh.2022/016
1 Pediatric Surgery Unit, Department of Surgery, Enugu State University Teaching Hospital, Enugu, Nigeria.
2 Neurosurgery Unit, Department of Surgery, Enugu State University Teaching Hospital, Enugu, Nigeria.
*Corresponding Author: Chukwubuike Kevin Emeka, Pediatric Surgery Unit, Department of Surgery, Enugu State University Teaching Hospital, Enugu, Nigeria.
Citation: Chukwubuike Kevin Emeka and Ozor Ignatius Ikemefuna (2022) A Study on the Incidence of Congenital Musculoskeletal Anomalies in a Tertiary Hospital in Enugu, Nigeria. J. Clinical Pediatrics and Mother Health, 2(1); DOI: 10.31579/jcpmh.2022/016
Copyright: © 2022 Chukwubuike Kevin Emeka, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 October 2021 | Accepted: 29 December 2021 | Published: 06 January 2022
Keywords: congenital; birth defects; musculoskeletal; tertiary hospital
Background:Congenital musculoskeletal anomalies refer to anomalies affecting the skeletal and muscular systems present when the child was born. In Nigeria, congenital anomaly of the musculoskeletal system is rarely reported. The aim of this study was to determine the incidence and distribution of clinically obvious congenital musculoskeletal anomalies among live born neonates at a teaching hospital in Enugu, Nigeria.
Materials and Methods:This was a retrospective study carried out on neonates at a teaching hospital in Enugu. The newborns were examined for congenital musculoskeletal anomalies and the study covered a period from 2016 to 2020.
Results: There were 7, 011 babies delivered in the teaching hospital during the study period. Overall, 109 babies had at least one congenital anomaly which gave an overall incidence of all congenital anomalies of 1.6% or 16 babies per 1000 live births. Out of the 109 babies that had congenital anomalies, 49 babies had a musculoskeletal anomaly. This gave an incidence of 0.7% or 7 babies per 1000 live births. There was male predominance and about half of the babies were delivered preterm. Syndactyly and polydactyly were the most common congenital musculoskeletal anomalies. Majority of the mothers were older than 35 years and were delivered vaginally. Two-thirds of the mothers had maternal illness during pregnancy and one-tenth had a previous history of congenital anomaly.
Conclusion:Congenital musculoskeletal anomalies are seldom reported. Polydactyly, syndactyly and talipes are the commonly seen anomalies.
Congenital anomalies or malformations, also known as birth defects, may be defined as structural defects present at birth which may lead to physical and mental disabilities [1]. Congenital anomalies represent defects in morphogenesis during early fetal life [2]. In developing and developed countries, congenital anomaly is a significant cause of infant morbidity and mortality. Although in poorer countries, malnutrition and infections take prominence [2]. In Asia, congenital anomalies account for 8-15% of perinatal deaths and 13-16% of neonatal deaths [1, 3]. Congenital musculoskeletal anomalies refer to anomalies affecting the skeletal and muscular systems present when the child was born. Multiple congenital anomalies can occur in a neonate and present a difficult challenge to the clinician [2]. The etiology of congenital anomalies is believed to be
multifactorial attributable to faulty development due to complex interaction of genetic and environmental factors [1]. Exposure to various teratogens during intrauterine life may affect the developing fetus resulting in permanent postnatal damage. Some of the teratogens include radiations, thalidomide and certain infections such as rubella [1]. Maternal age, parity, and antenatal illness are associated with congenital malformations [4]. The overall incidence of the entire spectrum of congenital anomalies has been quoted as 2% of total births [5]. Some studies have reported congenital anomalies of the musculoskeletal system as the most commonly [6, 7]. Available data on congenital musculoskeletal anomalies in sub-Saharan Africa are sparse. This study was an attempt to determine the incidence and distribution of clinically obvious congenital musculoskeletal anomalies among live born neonates at a teaching hospital in Enugu, Nigeria.
This was an observational study carried out at Enugu State University Teaching Hospital (ESUTH), Enugu, Nigeria. The hospital serves the whole of Enugu State, which according to the 2016 estimates of the National Population Commission and Nigerian National Bureau of Statistics, has a population of about 4 million people and a population density of 616.0/km2. The hospital also receives referrals from its neighboring states. Ethical approval was obtained from the ethics and research committees of the hospitals and informed consent was obtained from the patients’ mothers. For the purposes of this study, our interest was on clinically obvious and observable abnormality of musculoskeletal system which was noticed at birth or a few days after birth. All the live babies born in ESUTH during the period of this study were included. Stillborns were excluded from this study. This study covered a period of 5 years, from January 2016 to December 2020.
The protocol of this study conforms to the declaration of Helsinki. All the consecutive children who were born in ESUTH during the study period had a thorough physical examination (general and systemic) performed by a pediatrician and a pediatric surgeon at birth and at 6 weeks postnatal visit. This 2-stage physical examination minimized the error of missing any congenital anomalies of the musculoskeletal system. Diagnosis of congenital anomalies of the musculoskeletal system was based only on clinical evaluation of the babies by the pediatrician and pediatric surgeon. Investigations such as radiography, ultrasonography, and computed tomography scan and magnetic resonance imaging of the skeletal system were not performed.
For each patient, the following data were collected: gender, age of the baby at the time of diagnosis, maternal age, gestational age of the pregnancy before delivery (term/preterm), baby’s birth weight and mode of delivery. Baby’s birth weight greater or equal to 2.5 kilograms (kg) were considered to be normal while birth weight less than 2.5 kg were considered as low birth weight. Babies born at less than 37 completed weeks, calculated from the first day of last menstrual period, were considered preterm while babies born at or after 37 completed weeks were considered term. Other data collected include family history of congenital anomaly, maternal comorbidities such as diabetes/hypertension and use of herbs in early pregnancy.
Data Analysis
Statistical Package for Social Science (SPSS) for Windows version 23 (IBM Corp., Armonk, NY) was used for data entry and analysis. Data were expressed as percentages, medians and means.
3.1 Patents’ demographics
A total of 7, 011 babies were delivered during the study period, out of this number 109 had one congenital anomaly or the other. This gives an overall incidence of all congenital anomalies of 1.6% or 16 babies per 1000 live births. Out of the 109 babies that had congenital anomalies, 49 babies had a musculoskeletal anomaly. This gave an incidence of 0.7% or 7 babies per 1000 live births. Congenital anomalies of the musculoskeletal system accounted for 38.9% of all the systems.
There were 31 (63.3%) males and 18 (36.7%) females. The mean age of the neonates at diagnosis was 21 days. Twenty eight (57.1%) babies were term and 21 (42.9%) were preterm babies. Twenty-five (51%) babies weighed 2.5 kilograms and above while 24 (49%) babies weighed less than 2.5 kilograms.
3.2. Distribution of congenital musculoskeletal anomalies (n=49)
This illustrated in Table 1.

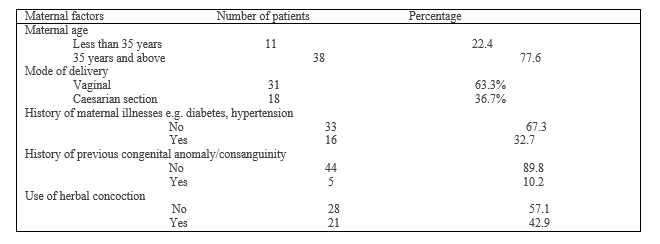
3.3. Maternal parameters
The possible maternal variables are shown in Table 2.
3.4. Prenatal diagnosis
Four (8.2%) patients had their musculoskeletal anomaly diagnosed prenatally during antenatal ultrasound scan. Two were polydactyly and the other 2 were talipes.
Interest in congenital malformations goes back to the dawn of history. William Harvey in his study on the possible causes of congenital malformations documented the teratologic phenomena and disturbance of fetal development [8]. According to the World Health Organization (WHO) document of 1972, congenital malformation should be confined to structural defect that are at birth [9]. However, in 2012, WHO included structural and functional anomalies including metabolic disorders as congenital abnormalities [10]. Our interest in the present study is on the structural musculoskeletal defects that are present at birth.
The overall incidence of congenital anomalies documented in the current study is comparable to the report of other series on congenital anomalies [10, 11]. However, other authors reported lower and higher incidence rates of congenital anomalies [12, 13]. The difference in incidence rates may be due to the discrepancies in detailed search and investigations performed for congenital anomalies in the different studies. The specific type of congenital anomaly may also determine its incidence. The incidence of congenital anomalies may vary over time or with geographical location [10].
Congenital musculoskeletal anomalies accounted for about one-third of all the anomalies in the current study and this is consistent with the report of Agrawal et al [1]. One study from Iraq reported musculoskeletal anomaly as accounting for one-fourth of all congenital anomalies [12]. The setting and period of the study may explain these differences. There are temporal and spatial differences in specific types of congenital anomalies. Congenital anomalies of the musculoskeletal system can be as high as 40% of all the anomalies [14].
Syndactyly and polydactyl were the most common congenital musculoskeletal anomalies recorded in the present study. This finding is in agreement with the report of a study from Korea [15]. Howbeit, other studies reported talipes as the most common [4, 10]. Daldrup et al reported dislocation of the hip as the most common congenital musculoskeletal anomaly [16]. The age group of the patients assessed may determine the predominant musculoskeletal anomaly obtained. For instance, talipes equinovarus may not be classically evident at birth but becomes more obvious as the child stands and begins to walk. In comparison, polydactyly is easily noticed even by the child’s parents.
In the current study, majority of the mothers whose children had musculoskeletal anomalies were older than 35 years. One study from Latvia reported that the prevalence rate of congenital anomalies increased depending on the maternal age [17]. The authors documented that there is higher proportion of preterm births and low birth weights among mothers aged 35 years and above [17]. Ironically, Goetzinger et al reported that advanced maternal age is associated with overall decreased risk for major congenital anomalies [18]. These findings may suggest that the “all or nothing” phenomenon plays a robust role in embryonic development with advancing oocyte age, with anatomically normal fetuses more likely to survive [18]. About two-thirds of the babies with congenital musculoskeletal anomalies, in the index study, were delivered vaginally. Congenital musculoskeletal anomalies may not determine the method of delivery. The mode of delivery is determined by obstetric, maternal and fetal concerns.
Maternal illnesses such as gestational diabetes mellitus and hypertension may be involved in congenital anomalies. About one-third of the studied patients’ mothers had a history of one illness or the other. Giardina et al reported association between the fetus and the mother during intrauterine life; they reported that maternal diseases may have negative impact on the fetus [19]. Maternal diabetes has toxic effects on the development of the embryo and the risk of congenital malformation is increased by three- to four folds [20].
History of previous congenital anomaly/consanguinity is an important consideration when evaluating patients with congenital abnormalities. Ameen et al reported the relevance of maternal history of previous congenital anomalies and the risk of the progeny having congenital anomalies [13]. Most congenital anomalies may be sporadic as only 10% of our patients had a previous history of having had a baby with congenital anomalies.
About half of the mothers whose children had congenital musculoskeletal anomalies took some herbs during their pregnancy. Illamola et al reported the association between the use of herbal medicine during pregnancy and congenital malformations [21]. Laelago reported that most of the women took the herbal medicine in an effort to treat nausea and vomiting [22].
Congenital musculoskeletal anomalies may be diagnosed prenatally. Fordham et al reported that subtle musculoskeletal anomalies become more recognizable in the second and third trimester [23].
Congenital musculoskeletal anomalies are seldom reported. Polydactyly, syndactyly and talipes are the commonly seen anomalies. Gestational illness such as diabetes should be well treated before and during pregnancy. Intake of herbal concoctions by pregnant women is to be discouraged.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
