
Review Article | DOI: https://doi.org/10.31579/jcobs.19/002
*Corresponding Author: Richard J. Naftalin, Kings, BHF Centre of Research Excellence, School of Cardiovascular Medicine and Sciences, Faculty of Life Sciences & Medicine, UK.E-Mail: richard.naftalin@kcl.ac.uk
Citation: Richard JN, Shahad S (2019) A Physiological Basis for Simulation of the Alimentary Limb Condition after Roux-en-Y Gastric Bypass Surgery.J. Clinical Obesity and Beriatric Surgery 2(1): DOI: http://dx.doi.org/ 10.31579/jcobs.19/002
Copyright: © 2019 Richard JN. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 October 2019 | Accepted: 25 October 2019 | Published: 07 November 2019
Keywords: roux-en-y gastric bypass; gastroesophageal reflux disease; gastric bypass weight-loss surgery
In England 26.2% of adults are considered obese BMI≥30 and a further 35.2% are overweight BMI≥25. Furthermore, around 30% of children aged 2 to 15 were classed as obese or overweight [1]. Despite extensive knowledge regarding energy balance regulation, the pathophysiology of obesity is still poorly understood and a wide variety of factors including genetic, behavioral and psychological factors are likely to play a role. Currently, the only effective treatment leading to significant and maintained weight loss, as well as a reduction in obesity-associated diseases, is bariatric surgery. The most effective type of bariatric surgery is Roux-en-Y gastric bypass (RYGB); though this is both expensive, costing around £30000 per patient, in U.K. and is associated with a high rate of post-operative complications, approximately 21% [11].This paper aims to summarise the main metabolic changes that occur post-RYGB that contribute to significant and maintained weight loss and to explore possible non-surgical medical therapies that could mimic the clinical and physiological effects of surgery.
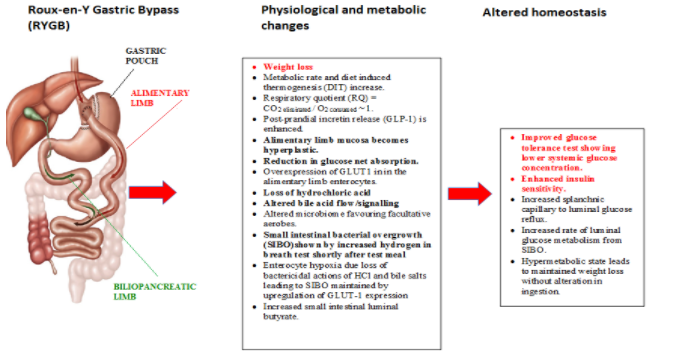
Obesity has become a global epidemic and has been shown to increase the risk of type 2 diabetes, hypertension, stroke, coronary heart disease, certain cancers, infertility and many other chronic disease conditions. Furthermore, obese patients seeking treatment were found to have an increased prevalence of psychiatric conditions, most commonly depression. This is associated with poor body image and low self-esteem resulting in a poor quality of life. Unfortunately, diet therapies are largely ineffective and although may cause weight loss in the short term, most, if not all, of the weight lost is regained [3,4]. Currently the only clinically effective treatment for obesity is bariatric surgery. Several types of bariatric surgery are employed in treatment of severe obesity, BMI≥40 [5]. Of these, Roux-en-Y gastric bypass (RYGB) is the most effective; [6,7,8] during the procedure the body of the stomach is isolated and the jejunum is anastomosed to the cardiac end of the oesophagus and gastric remnant. A biliary limb (BL) which includes the bile and pancreatic ducts, and occluded at isolated stomach end drains via the duodenum, into the jejunum at a distance from the newly established alimentary limb (AL) to form the biliary limb of the R en Y circuit. This operation prevents mixing of the AL content with gastric juice, bile salts and pancreatic enzymes [9] until it enters the common limb, Figure 1.
RYGB has been shown to cause a permanent reduction in body weight, with studies reporting weight loss of up to 70% of excess body weight [10,11] that continues for more than five years[6]. As well as causing significant and maintained weight loss in 80% of severely obese patients RYGB improves glycaemic control and results in the resolution of type 2 diabetes mellitus [12]. This is further supported by improved glucose tolerance tests taken post-operatively that show lower systemic glucose concentration with enhanced insulin sensitivity and a reduced insulin to glucose ratio in peripheral blood [13.14]
However, there are short and long-term complications that need to be considered. The most serious being anastomotic leaks, bleeding, venous thromboembolisms, including pulmonary embolisms and post-operative sepsis [15]. The incidence of an anastomotic leak post-RYGB is around 4.4% and is associated with a death rate of up to 30% [16]. Less serious complications include long-term nutritional deficiencies, which can occur months to years post-op [17]. Interestingly, even after being prescribed multivitamins post-RYGB, 37% of patients were still found to have vitamin B12 deficiency [16].
Previously it was thought that the significant weight loss and the remission of obesity-related diseases observed post-RYGB was solely the result of the calorie restrictive and malabsorptive aspects of the procedure. However, evidence suggests that appetite and food intake are not notably diminished following RYGB [18] and that in fact the underlying cause of post-operative sustained weight loss is due to complex metabolic and physiological changes.
Glucose homeostasis post-RYGB
The small intestine plays a major role in glycaemia control. Not only does it digest carbohydrates to glucose and transport glucose to the portal circulation, it also has an endocrine role by secreting hormones involved in glucose-mediated insulin release. Post-prandial levels of the hormone glucagon-like peptide 1 (GLP-1) increase post-RYGB [19]. GLP-1 is an incretin hormone that is produced by enteroendocrine cells found throughout the intestinal epithelium. Although the main role of GLP-1 is to stimulate insulin release, it also decreases glucagon production, as well as delaying gastric emptying and intestinal transit time [20]. Incretin levels are thought to increase as a result of the enhanced rates of food entry to the AL resulting from ablation of the pyloric sphincter and lack of gastric inhibition [21,22]. Although the increase in GLP-1 may play a role in improving glycaemic control, it cannot be the sole factor. A study looking at the role of GLP-1 in RYGB, found that in mice with a genetic loss of GLP-1 function, weight loss and improvement in glucose regulation was still observed post-RYGB [23].
In 2009, Stearns et al. were the first to show that remodeling of the gastrointestinal tract takes place after RYGB [24]. The alimentary limb (AL) becomes hyperplastic and hypertrophic, with both the villus height and crypt depth increasing in the AL but not in the BL of operated rats. Several other papers have documented similar changes, suggesting that they occur as early as 2 weeks post-RYGB [25,26,14]. Expression of the sodium dependent cotransporter (SGLT-1) after RYGB shows variable results. Some studies reporting a reduction in SGLT-1 mediated glucose uptake by up to 63% [24] whilst others have found an increase in SLGT-1 expression [22]. This heterogeneity in results may partly be due different the times at which these measurements were taken after surgery.
The hyperplastic changes observed in the AL are associated with overexpression of GLUT1 in the basolateral and apical membranes of the AL enterocytes [27.28]. Following RYGB, GLUT1 expression is observed in the jejunal mucosa, where it is normally only found during fetal development [29], increases the capillary to luminal glucose flow. Normally splanchnic capillary blood glucose concentration is higher than intestinal luminal glucose concentration [30]. The excess splanchnic glucose concentration arises primarily from SGLT1 activity across the enterocyte brush border membrane and absence of passive glucose transporters in the enterocyte apical membranes, which prevents glucose reflux into the intestinal lumen. However, reduction in luminal glucose can also occur secondarily to intestinal luminal glucose metabolism, due in part to small intestinal bacterial overgrowth (SIBO) [31] and in part to enterocyte gluconeogenesis [14.32], which consume luminal and enterocyte glucose. Figure 2.

depleted within hyperplastic alimentary limb. The overexpression of basolateral and apical membrane GLUT1 increases glucose uptake within the AL to provide the required additional energy to the hyperplastic AL [38]. Increased microbial aerobic glycolysis also leads to enterocyte hypoxia [39]. Increased microbial aerobic glycolysis within the small intestine could possibly be a result of increased aerophagia [25,40], due to the loss of the pyloric sphincter from RYGB, permitting more oxygen into small intestine and thereby increase aerobic bacterial metabolism [41]. Likewise, increased glucose shunting from splanchnic circulation via GLUT1 [14,25] could provide substrate for microbial aerobic glycolysis and maintenance of high luminal bacterial counts when digestate is absent from the small intestine lumen.
In addition to up-regulation of GLUT1, levels of enterocyte cytoplasmic hexokinase II were also found to increase post-RYGB [25]. These changes occurring exclusively in the AL [14,22,25] have been corroborated by positron emission tomographic human clinical studies showing enhanced metabolism of fluorodeoxy-D-glucose within the AL post-RYGB.
Factors involved in post-RYGB weight loss
a) The microbiome
Bariatric surgery alters the microbiome to favour facultative aerobes. Normally, obese individuals have an increased Firmicutes: Bacteroides ratio, however following medical weight loss and bariatric surgery, this ratio decreases, resembling the gut microbiome seen in lean individuals [42,43]. Conditions that favour a shift in the small intestinal microbiome include aerophagia [41], SIBO [44,45] loss of intrinsic disinfectants namely hydrochloric acid [46,47] , and diversion of bile from the alimentary limb [48]. As mentioned above, aerophagia may be due to the loss of the pyloric sphincter permitting more oxygen into small intestine [41]. As for SIBO, it is known that SIBO occurs post-RYGB [49,50,51,52] as confirmed by an increase in hydrogen in breath tests measured shortly after a test meal [53,54]. SIBO results in inflammation that induces enterocyte hypoxia [55,56], demonstrated by the raised enterocyte expression of HIF1, as well as mammalian target of rapamycin complex 1 and 2 (mTORC1 & 2) [14,47], and increased enterocyte NADH [25,58]. Additionally, SIBO produces butyrate, which has been shown to reduce weight gain and improve glucose homeostasis and insulin sensitivity in murine models [59,60,61]. Butyrate’s mode of action is still not fully understood, though it is thought to involve the promotion of energy expenditure and mitochondrial function [59]. It has also been shown to stimulate the secretion of GLP-1 and GLP-2 through a signalling cascade initiated by proglucagon mRNA, as well as enhance gene expression of GLUT-2 and increase both hexokinase and glucokinase activity and expression [62]. Furthermore, butyrate has been shown to increase the length and weight of the intestine, as well as increase villous height and goblet cell count and therefore may be responsible for the local hyperplasia observed in AL post-RYGB [63].
b) Gastric HCl secretion
During RYGB, a large portion of the acid secreting gastric mucosa is excluded from the alimentary limb, resulting in a post-RYGB decrease hydrochloric delivery to the alimentary limb. This depletion of hydrochloric acid contributes to changes in the gut microbiome. Gastrin secretion was found to be reduced post-RYGB [64]. The reduced acid content of the alimentary limb post-RYGB favours the survival of acid-sensitive microorganisms and promotes the growth of facultative anaerobes within the firmicutes phylum [44].
c) Bile acids
Removal of bile from contact with AL lumen has several important consequences; in addition to impairing and delaying lipid digestion and absorption, there is a close relationship between bile acids and the gut microbiota. Bile acids have antimicrobial properties that can affect the colonization of the gut microbiota. Thus, absence of bile will promote SIBO in the AL. Conversely, the gut microbiota contributes to the biosynthesis and biotransformation of bile acids. Serum bile acid level increases post-RYGB by up to twofold when compared to lean and obese individuals [65]. This is thought to be a result of the altered gastrointestinal anatomy. A study by Kohli et al, where a catheter was placed in the common bile duct of male obese rats to drain bile to the jejunum [66], resulting in a short-circuiting of the enterohepatic bile acid circulation showed an increase in serum bile acids and increased secretion of the hormone GLP- 1 and improved glucose tolerance [67]. Bile acids are thought to improve glucose tolerance and increase GLP-1 production by binding to the nuclear receptor FXR and the cell surface receptor, TGR5 [68].
Diet induced thermogenesis and metabolic rate
Energy expenditure (EE) of patients increases post-RYGB [69]. These post-RYGB metabolic changes may play a key role in maintaining weight loss. Studies have suggested that gut hyperplasia together with changes in bile flow, incretin secretion and increased intraluminal glucose metabolism [14,25] all contribute to the increase in EE [70]. EE was found to increase at rest and particularly in the post-prandial period, suggesting an increase in diet induced thermogenesis (DIT) [69,70,71]. DIT is the energy spent on digestion and absorption of nutrients; obese individuals tend to have a low DIT [72]. The low DIT observed in obese individuals may be due to reduced activation of the sympathetic nervous system, which is involved in thermoregulation [73]. Whereas post-RYGB, sympathetic nervous system activity has been found to increase [74], which has been suggested as a possible explanation for the increased DIT. The increase in DIT was associated with a raised respiratory quotient RQ= CO2 exhaled: O2 consumed ~ 1; implying that more carbohydrate is metabolised [63,64,71].The increase in carbohydrate metabolism may be secondary to the enhanced production of GLP-1 and thus the release of insulin post- RYGB [75]. Another and probably most likely cause of increased post-prandial DIT after RYGB is enhanced intraluminal microbial metabolism induced by the surge in substrate supply both from the ingested materials within the lumen and from glucose reflux from the splanchnic circulation. Nevertheless, along with all the changes mentioned in this paper, the increase in EE and DIT observed post-RYGB could be one of main contributing factors to significant and sustained weight loss.
Conclusion and medical therapy
In conclusion, prolonged weight loss post-RYGB is initiated by SIBO resulting from loss of intrinsic gastrointestinal disinfectants, namely hydrochloric acid and bile salts from the alimentary limb. This is sustained by undigested food and glucose shunting from the splanchnic circulation, which reduces net glucose uptake. Net intestinal glucose uptake is reduced both as a result of increased intraluminal glucose consumption by facultative anaerobic bacteria and an increase in glucose reflux due to the upregulation of GLUT1 in the basolateral and apical membrane of enterocytes. These changes are associated with enterocyte hyperplasia and increased gluconeogenesis. A summary of the main changes that occur post-RYGB is shown in Figure 1.
There is the potential to replicate the pathophysiological mechanism pertaining to weight loss after bariatric surgery by applying pharmacological rather than surgical agencies. A combined therapy that reduces hydrochloric acid, alters bile acid flow and thereby promotes SIBO with consequent intraluminal butyrate formation with gut hyperplasia including GLUT1expression could result in weight loss and improved glucose control. Such a therapy could provide a safer and cheaper alternative to bariatric surgery, which would make it more accessible to a much wider population than the current surgical interventions allow.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
