AUCTORES
Globalize your Research

Case Report | DOI: https://doi.org/10.31579/2692-9759/086
1 Cardiology Department, University Hospital Mohamed Taher Maamouri, Nabeul.
2 Service anatomy pathologies, Hospital Abdurrahman Mami Ariana.
*Corresponding Author: Zeineb Ajra, Cardiology Department, University Hospital Mohamed Taher Maamouri, Nabeul.
Citation: Ajra Z., Ismail O., Hamdani A., Khannouch A., Gheni R., (2024), A Giant Left Atrial Myxoma, Cardiology Research and Reports. 6(7); DOI:10.31579/2692-9759/086
Copyright: © 2024, Zeineb Ajra. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 December 2024 | Accepted: 12 December 2024 | Published: 23 December 2024
Keywords: AIS; 52-year-old patient; heart rate
Although myxoma is the most common primary cardiac tumor in adults, it accounts for only 0.25% of all cardiac masses. Although benign from a histological point of view, its intracardiac localization can be life-threatening for the patient. Its insidious symptomatology often makes it difficult to diagnose until the stage of complications.
Although myxoma is the most common primary cardiac tumor in adults, it accounts for only 0.25% of all cardiac masses [1]. Although benign from a histological point of view, its intracardiac localization can be life-threatening for the patient. Its insidious symptomatology often makes it difficult to diagnose until the stage of complications [3]. About 50% of patients with myxomas present with symptoms of cerebral or peripheral embolism, or intracardiac obstruction, while ten percent are completely asymptomatic [1,2]. The risk of long-term recurrence requires a large resection, meticulous exploration of the four cavities and regular echocardiographic follow-up [1].
We report the case of a 52-year-old patient, with a history of hypertension (Irbesartan 300mg/Hydrochlorothiazide 12.5mg), dyslipidemia (atorvastatin 20), admitted to our department for management of angina pain to the effort with NYHA stage II dyspnea that had been evolving for a few weeks. The physical examination reveals a good general condition, the blood pressure is 110/60mmhg. Cardiac auscultation reveals a diastolic rolling at the mitral focus, pulmonary auscultation is free. The rest of the physical examination was without particularities. The electrocardiogram showed a regular sinus rhythm with a heart rate of 115 beats/min, left atrial enlargement and no sign of ischemia.
Transthoracic echocardiography (Figure 1) showed a dilated left atrium with a hyperechogenic mass measuring 31/28 mm transversely and 69/37 mm longitudinally, appended to the AIS, obstructive at times with a mean gradient over the mitral valve of 14 mmhg. LVOT was 60% and PAPS 76 mmhg.
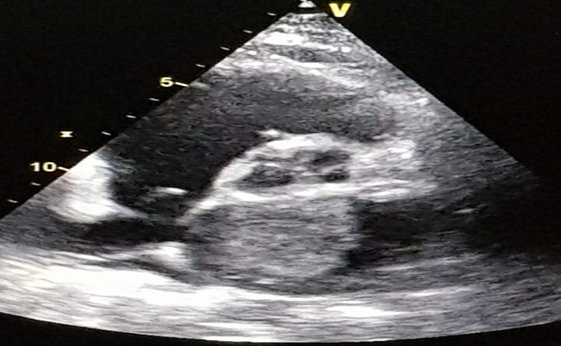
Figure 1: ETT left parasternal long axis showing a large hyperechogenic mass in the left atrium.
The patient was transferred the same day to the surgery department of Ariana for a complete resection of this tumour, the anatomopathological examination confirmed that it was a benign myxoma (figure 2a,2b).
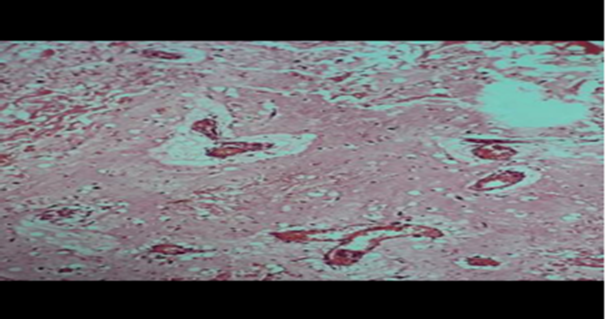
Figure 2a: low magnification: abundant myxoid stroma with rudimentary vascular structures and spindle or stellate cells
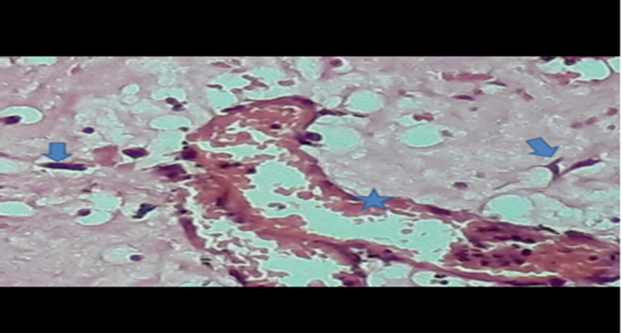
Figure 2b: high magnification
Arrows: spindle or stellate cells with eosinophilic cytoplasm and elongated nuclei without atypia
Asterix: rudimentary vascular structures
The postoperative phase was simple. The patient is regularly observed; she is totally asymptomatic. Cardiac echocardiography shows no recurrence of the mass.
Primary cardiac tumors represent less than 0.2% of all cardiac masses, three quarters of these tumors are benign and half of these tumors are myxomas, la femme est plus souvent touchée [3,5].
Myxomas can be found in the atria, the ventricles or on the mitral valve, with a predilection for the left atrium [4]; such is the case of our patient.
Intracardiac myxoma is a pathology which is characterized by a very large clinical polymorphism which can cause a diagnostic delay [4], in fact, the symptomatology can be correlated to the size of the tumor, to its location in relation to the mitral orifice. and to the pulmonary veins, to its appearance (gelatinous or fibrous) as well as to its mobility (villous or pedunculated tumor). Our patient presented on physical examination signs of mitral disease and signs of left heart failure on exertion.
Echocardiography has become the essential diagnostic exam for myxoma and the determination of its characteristics (location, base of implantation, shape, size, calcifications, etc.) [7], all times Transesophageal ultrasound, computed tomography and l MRI can also be used for diagnosis, especially
in cases of difficult differential diagnosis with an intracardiac thrombus being the main differential diagnosis. These exams also make it possible to differentiate from other intracardiac tumours [6].
Surgical resection with extracorporeal circulation is the only possible treatment for cardiac myxoma. This procedure consists of excision of the entire tumor removing the insertion base to prevent recurrences [8]. The anatomopathological study confirms the diagnosis and the benignity of this tumour.
The myxoma has a large clinical polymorphism, its obstructive form constitutes an urgent surgical indication because of the risks of enclavement.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.


























































