AUCTORES
Globalize your Research

Case Report | DOI: https://doi.org/10.31579/2641-0427/003
1. Centre for SPINE Surgery, MIOT Hospital, Chennai.
*Corresponding Author: Charanjit Singh Dhillon, Centre for SPINE Surgery, MIOT Hospital, Chennai.
Citation: Charanjit Singh Dhillon, Surgical management of symptomatic Adult lytic Spondyloptosis by modified/Three stage Gaines procedure: case report, J Orthopaedics and Surgical Sports Medicine.1(1); Doi: 10.31579/2641-0427/003.
Copyright: © 2018 Charanjit Singh Dhillon et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 May 2018 | Accepted: 29 June 2018 | Published: 16 July 2018
Keywords: spondyloptosis; lumbosacral kyphosis; corpectomy
Spondyloptosis or complete anterior dislocation of the L5 vertebrae over S1 is a rare clinical condition. Generally, the surgical management of spondyloptosis includes either posterior long segment in-situ fusion (with total disregard for altered biomechanics) or restoration of lumbosacral kyphosis by reduction of spondyloptosis using multi-staged procedures. Reduction is possible in spondyloptosis only after sacral dome osteotomy or L5 Corpectomy with interbody fusion of L4 over S1 as described by Robert Gaines. We present our case of a manual laborer who was treated successfully by modified/Three stage Gaines procedure.
Spondylolisthesis is a slipping of all or part of one vertebra forward on the other [1]. Meyerding, an obstetrician, described four degrees of slip in spondylolisthesis according to the slip percentage [2]. Grade III, IV and V (spondyloptosis) are collectively classified as High grade spondylolisthesis (HGS) with slip percentage more than 50% [3,4]. These comprise of total less than 5% of total spondylolisthesis with spondyloptosis being very rare (less than 1%) [3,5]. HGS respond poorly to conservative treatment and treatment of choice is often operative(3,4,5,6,7,8).
Spondyloptosis is defined as a condition were L5 vertebral body is completely dislocated from the sacrum anteriorly [6,7]. It was originally described by Neugebauer [9]. Patients usually display classical symptoms of low back pain, stiffness with hamstrings tightness without or with radicular symptoms or cauda equina syndrome [3,4,5,7]. Generally, the surgical management of spondyloptosis includes either posterior long segment in-situ fusion or reduction of spondyloptosis using multi-staged procedures. Traditional treatment by in situ posterolateral arthrodesis totally disregards the lumbosacral kyphosis and the altered lumbosacral biomechanics and has been associated with pseudarthrosis rates up to 50%. Even with successful posterolateral fusion, the graft is in an unfavorable biomechanical environment, owing to it being under tension, which can allow for progression of lumbosacral kyphosis (slip angle) and sagittal translation (slip). Open reduction of spondyloptosis after L5 Corpectomy(Gaines Procedure) improves the biomechanical situation by reducing lumbosacral kyphosis and restoring lumbosacral lordosis, but is associated with neurologic deficits in up to 30% of patients. We present our case of a manual laborer who was treated successfully by modified/Three stage Gaines procedure.
Case Report: A 29 year old male, manual laborer, presented to us with complaints of severe low back pain and bilateral sciatica. There was no history of trauma. He had spondyloptosis of L5 over S1 with modified Newman’s score of 10+10. The patient underwent three staged modified Gaines procedure to reduce L4 over S1 after anterior L5 Corpectomy to achieve restoration of Lumbosacral lordosis and strong interbody fusion between L4 and S1. The reduction was maintained at end of eighteen months and he was able to resume his job as manual laborer.
A 29 yr old male patient, manual laborer, presented to us with complaints of severe low back pain and bilateral sciatica. The low back pain was insidious in onset and gradually progressive. The pain worsened with all activities of daily living and improved partially with rest. He was unable to walk more than 500 meters at a stretch due to pain. There was no history of trauma preceding the onset of his symptoms. The Oswestry Disability index (ODI) score at the time of initial presentation was 70. He was given a trial of conservative management in form of analgesics, corset and activity modification for over 6 months. However he did not have any significant relief.
On examination, patient was unable to stand erect until he flexed his hips and knees. He had flattened buttocks, with severe hamstrings tightness and a positive step sign. Neurological examination revealed sensory blunting in bilateral L4 and L5 dermatome (50%) and weakness in right extensor hallucis longus (EHL) and right Tibialis anterior (TA) muscle (power 3/5).
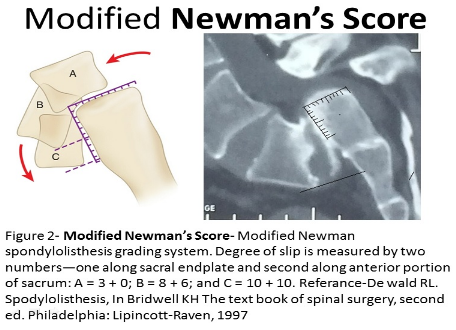
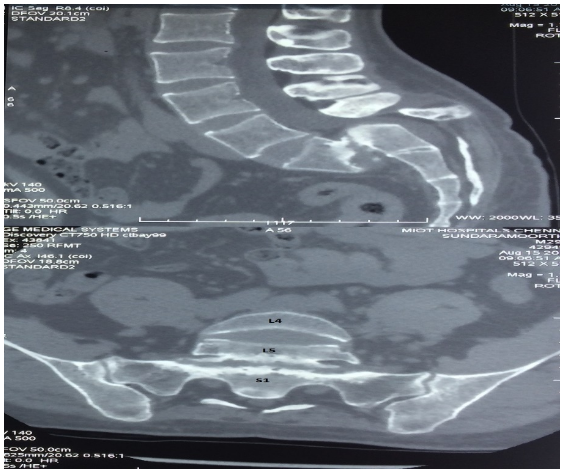
X-ray revealed spondyloptosis of L5 with the L5 superior end plate was lying below the S1 superior end plate (figure-1). The L5 vertebra has not just translated forward and dropped into pelvis but also rotated sagittal plane along transverse axis so that the inferior endplate of L5 was facing the anterior surface of S1 body. His modified Newman’s score was 10+10 (Figure-2). MRI Scan showed compression of the Dural sac at L5 S1 level with severe bilateral L5 neural foramina compression. CT scan showed unsuccessful attempts at natural fusion between inferior endplate of L5 and anterior surface of S1 in the form of developing osteophytes (Figure-3). Dynamic flexion and extension X-rays and traction X-rays showed no mobility at L5 S1 region.

The patient was counseled regarding various options for treatment including non-surgical management. The option of leaving the listhesis uncorrected with possibility of further worsening of neurological status was informed to patient. Frank discussions regarding the morbidity of surgery and the technical difficulties in obtaining reduction of spondyloptosis along with the possibility of worsening the preexisting right TA muscle weakness to complete foot drop and the possibility of retrograde ejaculation following anterior surgery was discussed with patient and his family in his native language. After thorough discussion with the patient and after fully understanding the pros and cons of operative procedure, he consented for surgery. A three staged anterior-posterior-anterior intervention was planned for reduction of spondyloptosis, in single session of anesthesia.
During first stage, anterior transperitoneal approach to L5 and S1 vertebra was done through Pfannenstiel incision. Major Neurovascular structures were dissected and secured by blunt dissection with the help of vascular surgeon. L5 body was identified. Complete L5 corpectomy up to base of pedicles was done along with excision of L4L5, L5S1 disc. Completeness of corpectomy was confirmed intra-operatively with image intensifier. Wound was closed temporarily in single layer and sterile dressings applied.
In second stage, with the patient in prone position, midline sub-periosteal exposure of spine was done from L2 to S2. Polyaxial pedicle screws of 6.5mm (Medtronics-Legacy) were inserted in L3, L4 pedicles on either side. Colorado sacral plate (Medtronics) with pedicle screws in S1 and alar screws in S2 was used to form base of the distal construct. All screws were inserted under fluoroscopic guidance. Posterior elements of L4 and L5 were excised and bilateral L4, L5 nerve roots were decompressed till they exited the neural foramina. Rods were firmly secured to sacral plate and gradual reduction of L4 over S1 was achieved without undue tension on the roots. Wound was closed in layers after complete hemostasis.
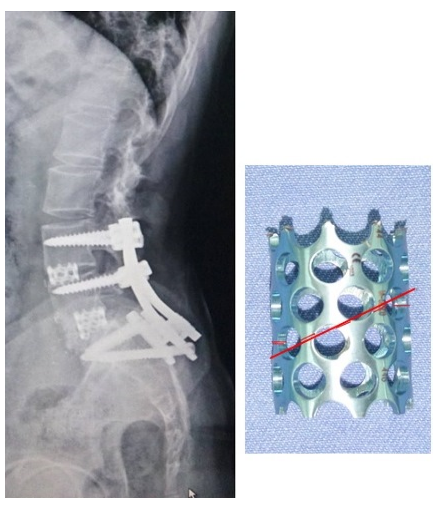
In third stage anterior abdominal wound was reopened. The empty corpectomy space was reconstructed with an appropriate size Harm’s prototype cage contoured in lordosis and filled with bone graft (figure-3). L3L4 disc space was identified and curetted and fused with cages filled with bone graft. The position of cage was confirmed by image intensifier. Stability of cages was checked intra-operatively. After complete hemostasis, wound was closed in layers over drain.
Patient was stable and withstood the surgical procedure without any hemodynamic complications. Nevertheless right EHL and right TA continued to remain weak in the immediate post-operative period (Pre-op right EHL and TA muscle power was 3/5). This was in spite of inspection of L4 and L5 roots during the reduction maneuver to prevent any undue nerve root tension.
The patient was mobilized after 48 hours with lumbar corset. He was instructed to walk with hips and knees slightly flexed for the first one month to reduce the traction on L4 and L5 nerve roots. Sutures were removed after 12th postoperative day and patient was discharged in stable condition. He was refrained from activities such as lifting weights, sitting cross legged, bending forwards for up to 6 months.
On regular follow-up, his right EHL and TA power improved gradually over a period of 6weeks and he was able to walk comfortably upto 2km by the end of 6 months. At the follow up of 18 months, he had significant symptomatic improvement with postoperative ODI score to 8. Radiology showed solid fusion with maintenance of sagittal balance (Figure-4).
He was able to return to his job as a manual laborer by 6 months (Figure-5).

Spondyloptosis or complete anterior dislocation of the L5 vertebral body over S1 is a rare clinical condition. It is perhaps the most challenging pathology faced by the spinal surgeon. The ideal method of treatment of this rare situation is still a subject of controversy. On one extreme are conservative surgeons who recommend posterior long segment in situ fusion with no attempt at reduction[10,11,12,13] while on the other extreme are adventurous surgeons who recommend partial or complete reduction of spondyloptosis and correction abnormal sagittal alignment with instrumentation (14,15,16,17). Reduction of forward translation of L5 over S1 is possible in cases were lower end plate of L5 vertebra is at, or above the level of Superior end plate of S1 vertebra. In severe cases, reduction can also attempted by sacral dome osteotomy [14]. However in our case, L5 superior end plate was lying below superior end plate of S1 vertebra into the pelvis, so reduction with sacral dome osteotomy was technically difficult.
In 1985, Gaines et al [15], popularized a two staged surgical technique for reduction of the spondyloptosis. In the first stage L5 vertebral body was excised up to the base of pedicles. The second stage under separate anesthesia was performed after few days wherein the loose neural arch and pedicle of L5 were removed from posterior approach with gradual reduction and docking of L4 over S1 achieving bone on bone contact, stabilized by transpedicular instrumentation [14, 15]. K Karla et al in 2010 reported a modified Gaines technique for case of spondyloptosis (patient with modified Newman’s criteria score of 10+6), where they performed partial L5 corpectomy and reduced the deformity [17]. In our patient the L5 vertebral body was displaced below the level of superior end plate of S1 with modified Newman’s score was 10+10 [16], hence reduction by partial corpectomy of L5 vertebra was difficult.
We modified Gaines procedure into three stages. The first stage was similar to that described by Gaines[15, 16]. In second stage, pedicle screws were inserted in L3 and L4. For sacral fixation, we deliberately used Colorado sacral plate with S1 sacral screw and S2 alar screw to use the combined strength of S1 pedicle and S2 alar screws to enhance distal fixation. L3 and L4 vertebral body were sequentially reduced to the distal sacral fixation. Due care was taken to observe the L4, L5 and S1 roots and to look for any tension on the nerve roots during reduction maneuver. In this case we were able to achieve complete reduction of L4 over S1 while maintaining lumbosacral lordosis.
In stage three, we had to bridge the corpectomy defect as well as we had to maintain lumbosacral lordosis of around 20 degrees that we had achieved in posterior reduction. Since, there was no such commercially available cage; we used Harm’s prototype cage of appropriate size which was customized to required lordosis by cutting the cage obliquely around the
circular lattice

Figure 6- Follow up at 18 months Post-op showing spine range of movements and TA recovery
In classical Gaines procedure the L4 vertebral body is directly docked on to the superior endplate of S1 achieving direct bone on bone fusion between L4 and S1 vertebral bodies. As a result there is no lordosis between L4 and S1 vertebral bodies. Also in between L4 and S1 pedicles there are two nerve roots (L4 and L5) exiting through the common foramina which are subject to overcrowding and compression since no cage is used between L4 and S1 vertebral bodies. In our case we were did not dock L4 vertebral body directly on S1 superior end plate but left considerable gap in between the two endplates to attain wider neural foramina height. The gap was reconstructed with a 20 degree lordotic cage to restore lumbosacral lordosis and thus ensuring better biomechanics at lumbosacral junction compared to classical Gaines procedure.
Foot drop is the most commonly reported complication in many studies, where reduction maneuver was performed [13, 14 ,15 16]. Hu SS in 1996 mentioned the rate of neurological complications of around 25% and complications such as root injury, cauda-equina syndrome, injury to hypogastric plexus during anterior procedure [19,20]. In Gaines study, 23 out of 30 patients had clinical deficit in L5 root following their reconstruction. However, 21 out of 23 patients in Gaines study having root deficits, recovered fully from 6 weeks to three years following their reconstruction [16]. According to DM Petraco, 71% of strain occurs on L5 nerve root in second half of reduction maneuver in high grade listhesis and correction of the lumbosacral kyphosis may be protective for L5 nerve root [18].
Our patient already had EHL and TA weakness over right side before surgery. The possibility of worsening of the neurology was discussed with the patient before surgery. In spite of close intraoperative monitoring for root tension there was no improvement in TA and EHL strength in the immediate post-op period. Nevertheless over a period of 6 months the patient recovered completely and was able to resume his work as manual laborer. At the end of 18 months of follow-up, our patient recovered clinically with ODI score of 8 from 70. Radiological parameters were measured using PACS (picture archiving and communication system) software and these parameters showed improvement to acceptable level (Table-1).
Pelvic Parameters | Pre-op (Degree) | Post-op (degree) |
Pelvic Incidence | 52 | 52 |
Pelvic Tilt | 27 | 19 |
Sacral Slope | 25 | 33 |
Lumbo-Sacral Angle | -7 (kyphosis) | 20 (lordosis) |
Table 1: Comparison of Pelvic parameters before and after surgery
The modified/Three stage Gaines procedure is technically safe and effective technique to correct the deformity, achieve lumbosacral lordosis and fusion in case of severe spondyloptosis, provided done with experienced hands. The use of a wedged interbody cage instead of direct bone on bone docking of L4 over S1 (as done in classical Gaines procedure) helps to reinstate lumbosacral lordosis restoring normal biomechanics and gain extra height of neural foramen between L4 and S1 pedicles where two exiting roots L4 and L5 are residing in the common lateral recess. Transient post-op L4 and L5 root neuropraxia is possible and the patient needs to be counseled regarding its possibility pre-operatively. However, this is an isolated case and need larger case series and long term follow-up for becoming a standard procedure in correcting such severe spondyloptosis.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.
