AUCTORES
Globalize your Research

Review Article | DOI: https://doi.org/10.31579/2578-8949/043
*Corresponding Author: Nastja Kučišec-Tepeš , Department of Croatian Wound Association, Zagreb, Croatia
Citation: Nastja Kučišec-Tepeš , Prevention of Chronic Wound Infection in Clinical Practice,.J. Dermatology and Dermatitits, DOI: 10.31579/2578-8949/043
Copyright: © 2018 Nastja Kučišec-Tepeš et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 June 2018 | Accepted: 22 August 2018 | Published: 07 September 2018
Keywords: prevention, infection, chronic wound, strategies, biofilm.
The notion of prevention includes all procedures by which a disease-infection is being inhibited and its development and spreading is halted.
For an efficient implementation of preventative procedures, we must be familiar with the basic comorbidity of the patient and treatment, phases of physiological healing of the wound, risk factors which cause delayed healing, pathophysiological features of the chronic wound, a continuous development of infection with a particular emphasis on biofilm.
Prevention of chronic wound infection includes a range of active procedures by which the development of infection and its progression is halted. The key moment is the recognition of the patient with a chronic wound in phase of colonization and with a timely intervention the development of infection is prevented.
We live in a modern world characterized by an increasing proportion of the elderly among the overall population, increase of body weight, malnutrition, diseases of the circulatory system, neoplasms, major surgical interventions in which ischaemia is the predominant risk factor.
The best wound care is the prevention of the development of the chronic wound, followed by prevention of infection which is the complication of the basic endogenous disease. Prevention of the chronic wound infection represents a successful management of the chronic contaminated or colonized wound.
Chronic wound infection can be prevented by a quality and targeted medical care provided it assists the physiological healing with an optimal immune response on the part of the host. At the same time, the number of microbes in the wound is reduced and active measures are undertaken to destroy the biofilm. In addition, it is unavoidable to carry out general preventive measures which will prevent a recolonization of the bacteria, and thereby the reconstruction of the biofilm.
The aims of the prevention are: to avert the development of infection as well as the spreading of a local into systemic infection and delay the onset of infection for as long as possible. The infection of the wound is defined by the quantity of microbial colony forming units (CFU) in gm/ml, overall virulence of the microbes with the domination of biofilm and the composition of the microbial community, all against the background of the immune response of the host, quantity of exudate and necrotic tissue.
Modern preventive procedures and methods are multimodal, because the infection is multi-factorial. The development of infection depends on the cumulative effect of risk factors in relation to the host’s defensive system.
Bacteria are the leading causative agents, and the biofilm as the virulence factor determines the infection and its chronicity. All types of bacteria develop biofilm, and it is not an exclusive feature of dominant agents such as Staphylococcus spp, Streptococcus pyogenes, Pseudomonas aeruginosa, anaerobes of the skin.
The approach to the prevention, care and treatment of the chronic wound must be holistic, whereby we perceive the patient as a whole, not only his wound.
Prevention or efficient management of the wound infection includes the optimization of the host’s immune response through the treatment of the basic disease and control of successfulness of the treatment. The reduction of the number of microbes in the wound is achieved by the application of aseptic techniques, hygiene of the hands, moisture control and the control of exudate. The optimization of the wound bed is achieved by means of efficient cleaning procedures, application of antibiofilm-active antiseptics, supportive dressings and debridement. General preventive measures include also the education of the patient, treatment plan, psychosocial assistance and team work.
The prevention and treatment of chronic infected wounds is still an area prone to confusion, especially in the light of knowledge about the role of biofilm.
It is crucial to know that the application of individual preventive procedures will not prevent the infection of a chronic wound. Prevention of infection also implies a successful management of the contaminated or colonized wound.
“Health is the state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” [1].
Under the notion of prevention, we imply all procedures with which a disease, in our case infection is being prevented and its development and spreading are disabled [1].
The word originates from the Latin word preventio which means to precede. In its broader sense the prevention of infection implies its suppression, recognition, treatment and patient care. So, the prevention of infection reflects the principles of best clinical practice. In order to achieve this, we use the procedures of observation, identification and risk assessment along with control and surveillance. All preventive procedures must be evidence-based and include representation, proof, causes, interventions and consequences [2].
The importance of the acute and chronic wound prevention of infection is also referred to the document issued by the World Health Organization in 2015, which also enumerates the essential principles of prevention [3].
In order to be able to carry out preventive procedures and measures, we must know the essential phases of the physiological healing of the wound, factors which hinder healing or cause a delay in the process, specific features of the chronic wound and a continuous development of infection. Prevention of the chronic wound infectioncontains a range of active measures with which the progression of the chronic wound and the development of local or systemic infection are disrupted [4]. Moreover it represents secondary prevention because it relates to the recognition of the patient in the phase of contamination or colonization of the wound, whereas a timely intervention halts the development of infection [5].
We apply preventive procedures only when we know what needs to be prevented and which process should be targeted by prevention [6].
Chronic wound is a wound whose process of healing is sluggish or which manifests time-wise an intermittent, delayed or completely obstructed healing.
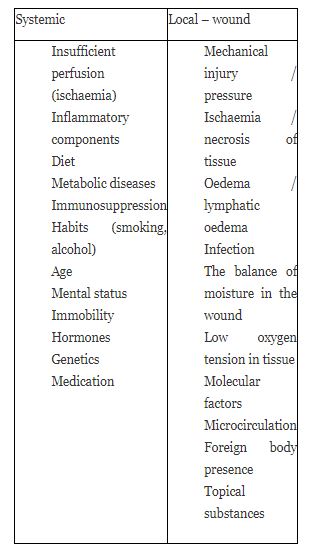
The definition of the Wound Healing Society is that a chronic wound is one which lags behind of an orderly and timely process of regeneration, one that would result in an anatomic and functional integrity. From clinical observation we can say that the chronic wound is one in which the healing lasts longer than three weeks [7]. The absence of healing depends on numerous intrinsic and extrinsic factors of the patient and wound itself. Today, a chronic non-healing wound is a paradigm for biofilm, a dominant virulent bacterial factor in the absence of healing and infection, whereby an underlying pathology such as ischaemia should be excluded (6,8). Complicating risk factors which hinder the healing are numerous and are shown in Table 1 (9,10).
Chronic wounds mainly develop from acute ones, when the physiological course of healing in any given phase is disrupted: this may occur in the haematostatic, inflammatory, proliferative or remodulating phase [13]. Finally, the chronic wound lags behind in the inflammatory phase which is characterized by high levels of proinflammatory cytokines [14,15].
At the same time, in the micro-environment of the wound, high levels of protease are present, along with a low level or protease inhibitors, whose ratio is key for successful healing [16, 24]. The result of the disbalance is the breakdown of the tissue matrix, reduction of growth factors and a drop of mitogenic activity [17,25]. When we add to this the activity of microbes, predominantly bacteria and their proteinases, the breakdown of the wound is complete [18].
The activity of bacterial proteinases is multi-potent and is manifested in the activation of matrix metalloproteinases (MMPs), toxins, degradation of extracellular matrix (ECM) protein and immunoglobulin, inactivation of proteinase inhibitors and a disbalance in the activation and inactivation of cytokines and complement factors [26]. On the molecular level, the processes create an ideal foundation for the spreading of infection and a delay in healing [3,19].
Chronic wounds are a present-day global epidemic [17]. For this reason, the primary aim is to prevent the development of the chronic wound, its progression and complications with an emphasis on infection (3,20-23). The treatment strategy is based on the establishment of cellular balance and a return of the wound into the healing phenotype, targeting etiological factors [17].
Infection of the chronic wound is an expected further complication , provided we accept the fact that the wound itself is a consequence of endogenous and exogenous pathophysiological processes along with the degeneration of the natural protective cover–skin [27, 37]. The consequence of infection is the absence of healing and an increase in the risk of loss of extremities or even of a lethal outcome. Between 2008 and 2016, significant advances were made in the scientific and clinical understanding of the chronic wound infection [27-37].
We live in a predominant world of microbes and human body itself contains around 1014 microbial units in its physiological flora. The physiological flora in man covers the skin and the mucosa, differing in its composition and concentration and plays an important role in the maintenance of health. When the balance between the microbes and macro-organisms is disrupted, conditions favourable for the development of infection arise [37, 38].
The etiologic agents of infection are predominantly bacteria, primarily gram-positive cocci, but in the chronic wound we also find gram-negative rods and anaerobes in varying combinations [42]. The proof of bacterial capability to excrete biofilm, along with the understanding of its influence and role in delayed healing, maintenance of chronicity, persistence of inflammation and development of infection, represent the greatest achievement of modern medicine related to the problem of chronic wound [6, 30-32].
Primary determinants of the pathophysiological process taking place in the wound are:
1.Quantity of microbes (bacteria) [33]
2.Type of bacteria which determines the type and quantity of virulence factors, with a predomination of biofilm [34-36, 87]
3.Ability of the host to defend itself from potential pathogens (immunocompetence) [6].
Table 2. Definition of wound infection (6,42)
Number of microbes + virulence + combination of bacteria
CFU/gm/mL biofilm aerobes / anaerobes
Host immune response + quantity of necrotic tissue + exudate
Table 2 : A summarized definition of wound infection is shown .
Chronic wound infection is a continuous process which develops in several stages and is defined by the relationship of microbes with the host.
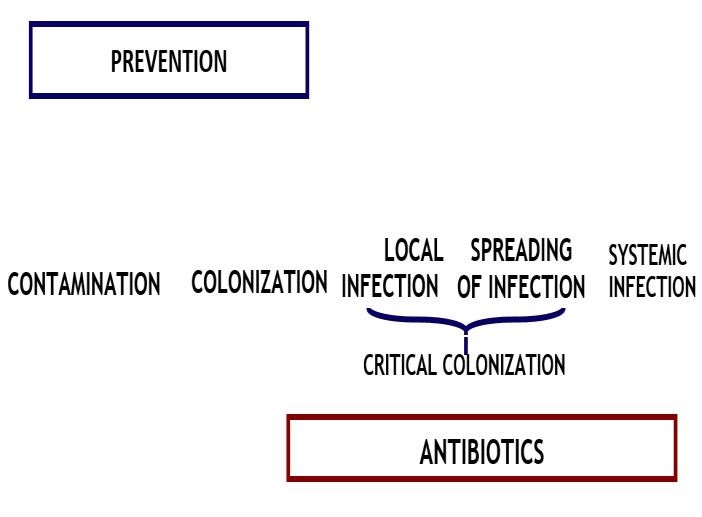
A continuous process of wound infection goes by several developmental stages: contamination, colonization, local infection, spreading of infection and systemic infection [40,41,43,44] (Fig 1).
These stages are characterized by clinical symptoms and developmental stages of microbes and biofilm (6, 98).
Having insight into the individual stages of chronic wound infection, along with a recognition of primary and secondary clinical signs of infection pointing to the biofilm, it is possible to implement
successful strategies for prevention, care and control [6, 27, 39].
For the understanding of individual stages of chronic wound infection, we apply the definitions accepted in 2016, which describe the relationship between the host, microbes and virulence factors (6). A brief description of the stages is the following:
Contaminants of the wound are members of exogenous and endogenous physiological flora including that from the environment, which appear as a consequence of poor hygiene, especially of hands and exposure to the environment. Essential preventive measures are: hygienic washing of hands, aseptic procedures, washing, rinsing, dressing, other procedures indicated by the appearance of the wound bed, the presence of exudate, risk factors and care of the wound’s environment [6, 45. 46].
All chronic wounds are colonized, but not necessarily infected. Colonization is a consequence of poor hand hygiene, absence of aseptic procedures and an incorrect application of dressings and antiseptics. Essential preventive measures: hand hygiene, aseptic procedures, firm cleaning and rinsing of the wound, sharp or filamentous debridement, dressing, taking care of the exudate.
The definition of critical colonization, due to lack of clarity and inherent vagueness, was broken down into local infection and the spreading of infection [40,43,48].
Preventive measures are belated or failed and the outcome of targeted treatment with antibiotics and debridement had a dubious action and outcome [43].
Continuity of development of chronic wound infection is caused by biofilm [6,19,30,49].
The recognition of biofilm as the dominant bacterial virulence factor and its developmental phases is essential for the strategies of prevention and treatment [43,50,51]. The goal of preventive and at the same time therapeutic procedures is the prevention of adherence of plankton bacteria to the destroyed surfaces of the wound-tissue, the destruction of the quorum sensing factor, prevention of phenotype changes in the bacteria, destruction of sessile bacteria and the disrupting of the renewal of biofilm with bacteria from the environment.
Stages in the development of biofilm are the following:
Prevention: destruction or killing of the microbes [52,53]
Enabled by the secretion of extracellular polymer substance (EPS) secreted by adhered microbes, which envelops the bacterial colonies. Prevention: destruction of EPS, quorum sensing molecules and adhesins [54,55].
After a successful irreversible attachment, the bacteria build a complex structure of a biofilm by means of the quorum sensing molecules. They organize the transport of nutrients, elimination of byproducts and control the density of bacterial population inside the biofilm along with the formation of microcolonies.
Prevention: destruction of quorum sensing molecules, specific receptors on the surfaces and adhesion [56].
Biofilm is structured in a complex formation. The defence of the host recognizes the biofilm. The result of the reaction is the presence of excessive number of neutrophils, pro-inflammatory cytokines and extensive secretion of host’s proteases. This, in turn, causes the destruction of tissue, significantly increased permeability of the capillaries and the development of oedema [53].
Prevention: combination of strategies along with the application of efficient biocides (antiseptics) and reduction of oedema [31].
A mature biofilm can be actively or passively dispersed / spread into the surrounding tissue. The main cause of spreading is an abundance of nutritive products on the wound’s surface.
Prevention: mechanical strong cleaning of the wound, sharp debridement, application of negative wound pressure therapy (NWPT), antibiofilm-active biocides and dressings, combination of procedures and methods indicated by the state of the wound bed, wound environment and the host [6,47,53,54,57].
It is significant that all types of bacteria and fungi in the wound are capable of forming a biofilm, not only the predominant agents of infection such as Staphylocccus spp, Streptocccus pyogenes, Pseudomonas aeruginosa, skin anaerobes [42].
The comprehensive care of the patient with a chronic wound must be such as to include all preventive procedures which will:
The procedures of prevention of infection have the following goals:
Understanding the risk factors, development of the wound, life cycle of microbes and features of the biofilm are a precondition for the application and carrying out of efficient preventive measures which will prevent the development of a chronic wound infection [6,11,21,60,98].
The factors related to the frequency of chronic wound infection are the following:
It is significant that the environmental factors in the patient are directly connected with medical care, depending on the knowledge and skill of medical personnel, as well as on the organization and financial capabilities to carry out the preventive and organizational strategies. [57-59].
The basic principles and goals in the prevention of wound infection have been accepted and applied for decades along with revisions and additions proceeding from scientific discoveries, clinical results and technological advancement.
The development of infection is multi-factorial and depends on the cumulative effects of risk factors related to the host’s defence mechanisms, along with external factors which increase the risk of wound infection. Bacteria are the predominant agents of infection, and virulent factors such as the biofilm determine the infection and chronicity [6]. For this reason, a holistic approach to care and treatment is mandatory, because in such an approach we observe the patient as a whole, not only the wound (Greek hólos = full, complete, whole). In order to reach the set goal, the cooperation of a multidisciplinary team is necessary, along with a comprehensive knowledge of risk factors, chronic wound development, continuity of infection and a recognition of biofilm as the predominant virulent bacterial factor [6,53,54,58,62]. Measures applied in prevention of infection are multimodal, meaning that no single measure is powerful enough to prevent such a complicated process [6,39,57].
We distinguish several types of measures which must be combined and repeated. These are:
Prevention of infection or a crucial preventive measure in averting local infection of the chronic wound is a recognition of delayed healing and progression of wound disintegration, because secondary clinical signs are not clearly visible [40,41].
Prevention of the spread of infection includes general, special and supportive measures along with an intensive repeated debridement and a targeted use of antibiotics. The applied antiseptics and dressings must possess anti-biofilm characteristics [39].
Integral skin, in anatomical and physiological sense, is the best prevention against the development of acute and chronic wound and infection. The skin possesses numerous functions, and some of them are the consequence of the presence and activity of physiological flora which colonizes the skin with numerous bacterial species. Molecular researches into the physiological flora have resulted in the discovery of biofilm and its role in the integral community and architecture of the skin [53].
Health Roadmap for Medical Research investigated the role of the biofilm of physiological microflora in the processes which characterize the physiological state of healthy skin, but also in the processes of absence of healing of wounds, chronicity and development of infection. In these researches the dominant agents of chronic wound infection were discovered, as well as the dominant virulence factor – the biofilm [63,64].
For the above reason, the care of integral skin is an essential factor in the prevention of wound development. This includes the risk factors, along with specific application of products, aids and materials [67-69].A general prevention is the hygiene of the skin along with moisture control and the application of medical lotions and creams [65].
The goal of preventive procedures is to avert the development of chronic wound infection, and thus to disable a continuous development of infection [6, 40]. Here it is of essence to prevent or reduce the influence of bacteria from the environment, such as hands, non-sterile objects and environment itself, as well as the physiological flora of the skin and mucosa in the patient [70].
The key procedures are hand hygiene, cleaning and rinsing of the wound, application of antiseptics and dressings with anti-biofilm activity and debridement [6,39,57].
Mechanical cleaning, irrigation and debridement open the “therapeutic window” for an efficient activity of antiseptics and dressings (Table 3)
Table 3: Therapeutic window (54)
sterile techniques
no-touch techniques
clean techniques (70,72,92,94)
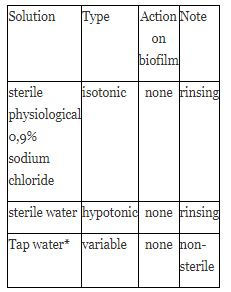
Decision to apply tap water is taken on the basis of water quality, immune competence of the
patient, characteristics of the wound (72,92)
All solutions before use must be warmed up to bodily temperature [73].
Antiseptics are surface-active substances of varied chemical composition. They are classified as drugs and are effective bactericides. They differ in the spectrum of activity on the microbe cell, efficiency, cytotoxicity, teratogenicity, induction of resistance and activity on the biofilm [77]. They are applied in the form of solutions, creams or are incorporated into dressings. They are used both in preventive and therapeutic settings.
The goals of preventive application of antiseptics on wounds are the following:
Targeted application of antiseptics in therapeutic purposes is to be a support to targeted treatment in cases such as:
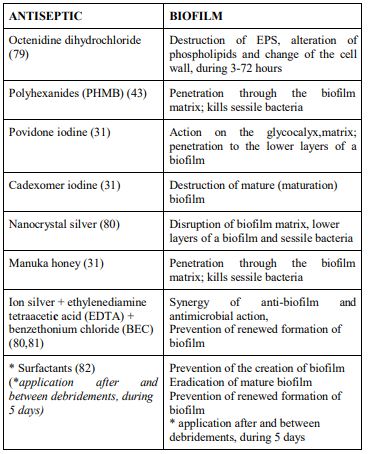
The reason for the use of antiseptics in preventive and therapeutic purposes is because there is no single therapeutic or preventive procedure which is effective on its own, but they must be combined. We ought to stress that there is no antiseptic which is efficient for all phases of development and forms of bacteria in the biofilm, which today is the paradigm for a chronic and chronic infected wound. For this reason, the application of a combined approach and use of different anti-biofilm active compounds is imperative [6,31,77] (Table 5).
With a reduction of the quantity of necrotic tissue and microbes in the wound, active substances can act as bactericides and anti-biofilm agents [54,89]. Cleaning of the wound is not always indicated for all types of wounds; the need and goal should be defined [75].
It is one of a procedures range which enables healing by reducing the quantity of microbes in the wound, controls and prevents wound infection, especially of the chronic wound, visualizes the wound bed and walls, and on the molecular level destroys the process of wound chronicity by lowering the levels of protease, cytokines as well as biofilm, and turns the wound from the chronic into acute one [88].
With regard to the era of biofilm it is good to orient oneself how much a certain type of debridement is successful as an anti-biofilm procedure (Table 6).
Debridement is a targeted procedure which plays a significant role in the prevention of the spreading of infection in the chronic wound. Efficacy depends on the timing, repetition of the procedure and change in the type of debridement. The latter depends on the state of the wound bed, walls and edges. The state of the wound is never static, it changes dynamically and should be carefully monitored and documented [78].
All types of debridement are efficient when applied immediately or on time, which is significant also in the light of its action on the biofilm [66,69].
Surface management of a wound is actually a manipulation with the aim of eliciting from the wound a positive response to the physiological process of healing. This type of care must be comprehensive and holistic in order to optimize the patient’s capability of healing through creating a physiological environment for the wound [6,39,57].
Prevention, as well as treatment of infected chronic wounds are still subject to a certain confusion, because the terminology used to describe the bacterial environment on the wound’s surface is still not clearly defined. For this reason, even the term “infection” should be redefined in the light of new knowledge about the presence and prevalence of the biofilm phenotype. The preventive procedures themselves must be assessed in accordance with the above [18].
Different definitions and descriptions of the techniques and procedures in the application of dressing in the context of wound care often also lead to confusion. The terminology used varies and often depends on individual interpretation. Therefore, it is justifiable to ask the question about the meaning of clean, versus sterile techniques in wound care [92]. This is especially important in the application of dressing [93].
There are no definitive data which would prove that sterile techniques are superior to clean ones in the care of chronic wounds, because the data are still insufficient to differentiate the incidence of infection [92]. Dominant disputes relate to the infected chronic wound and decubitus where the issue is being raised on the recolonization of bacteria and renewed formation of biofilm (95). In addition, a dispute is going on about the use of tap water by contrast to sterile physiological solution, in the context of frequency of infection. For the moment, a difference between the two means in the application on chronic wounds has not been proven (92).
Discussion is going on also about the use of sterile and non-sterile gloves. The factors which determine the choice between the two are: type of wound, exposed bone or tendon, immunosuppression, and non-specific ones are: knowledge, education, type of dressing, drainage (96).
The use of clean techniques in wound care saves time, whereas a higher incidence of infection in comparison to sterile techniques has not been proven (92,96).
We also find a certain controversy in the definition of the chronic wound infection with regard to clinical symptoms and microbiological findings concerning the biofilm (27).
The quantity of microbes expressed as CFU in g of tissue or the quantity of exudate of ≥105 CFU/g/mL is nowadays taken to be questionable in the definition of chronic wound infection. The question also arises in relation to biofilm as well as the agents of infection Streptococcus pyogenes, Clostridium spp (42).
As regards the biofilm, classical microbiological diagnostic procedures are inefficient. The infection is present and causative agents are trapped within the biofilm structure and escape microscopic proof and cultivation. The result of a classical microbiological examination: preparation stained according to Gram without visible microbes, culture is sterile and targeted antimicrobial therapy inefficient (27). Today, the presence of biofilm is being proven by qualitative and quantitative methods, the speed and strength of adhesion along with the sensitivity to antibiotics and antiseptics, depending on the type of bacterium. In this process, various cultivation methods are used (TCP, TM, CRA), latex agglutination, bioluminescent and molecular methods (ESEM) (99,100,101).
Unfortunately, all of the above is still not available in daily clinical practice [6]. Therefore, the chronic wound infection should be defined as the presence of bacteria in any given quantity, provided the secondary clinical symptoms of infection are present, the breakdown of the wound progresses and healing is delayed [84,92,97].
Concluding, we wish to raise the question whether a mere removal of microbes is sufficient for healing and whether it is a proof of efficacy of the topic antimicrobial substance (dressing). The relation of the total quantity of microbes, inflammatory response and clinical outcome is perceived to be of essence [22].
There are as yet no clinical data that only the application of antiseptics will prevent the infection of a chronic wound, and a recurrence of infection [22,27]. The same is true for all other preventive procedures taken individually.
The basic process in the prevention of chronic wound infection is the standardization of educational programs for all medical personnel which takes care of the wound. When a general consensus is reached, minimal educational programs should be defined [67].
In the light of multiple resistance of bacteria to antibiotics, it is of essence to undertake all preventive measures in order to arrest the development of infection in the chronic wound, because in such a manner treatment is made possible without the use of antibiotics.
The prevention of chronic wound infection is multimodal, because the presenting factors are numerous, with a predomination of biofilm. The basic preventive measure is “clean hands – clean wound”. Therefore, medical care must be comprehensive and holistic in order to optimize the patient’s capability of healing and to create a physiological environment around an acute wound. The application of preventive procedures results in a successful care of an infected chronic wound or an efficient management of the same. The key to prevention is the recognition of the colonization of a chronic wound and immediate multimodal preventive action.
We expect the future researches to focus predominantly on biofilm. This includes diagnostic tests for clinical use, understanding of the efficacy of debridement in the destruction of biofilm and its efficient removal with the breakdown of quorum sensing molecules.
“The prevention of infection lies in a successful care of contaminated or colonized chronic wound”.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.
